Jaeger Philippa, Toskas Ioannis, Henes Jessica-Kristin, Shcherbyna Serhii, Schwarz Frederic, Euper Miriam, Seizer Peter, Langer Harald, May Andreas E, Geisler Tobias, Gawaz Meinrad, Schreieck Jürgen, Rath Dominik
Department of Cardiology and Angiology, University Hospital Tübingen, Tübingen, Germany.
Departmen of Cardiology and Angiology, Ostalb-Klinikum, Aalen, Germany.
Clin Res Cardiol. 2025 Feb;114(2):203-214. doi: 10.1007/s00392-024-02442-1. Epub 2024 Apr 2.
Data on associations of invasively determined hemodynamic parameters with procedural success and outcomes in patients suffering from mitral regurgitation (MR) undergoing transcatheter edge-to-edge repair of the mitral valve (M-TEER) is limited.
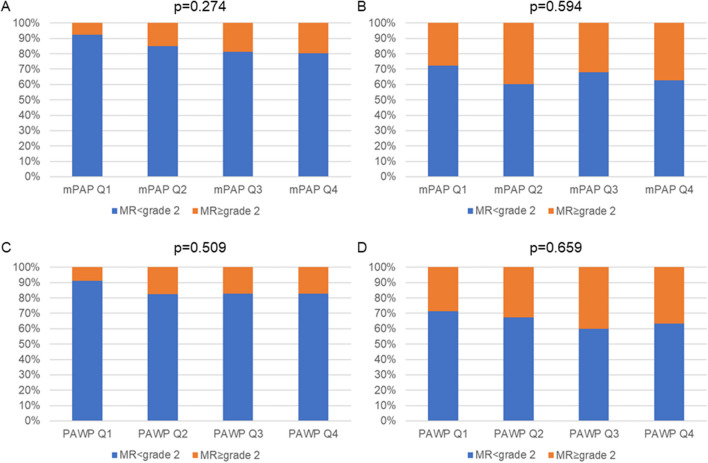
We enrolled 239 patients with symptomatic MR of grade 2 + , who received M-TEER. All patients underwent extensive pre-interventional invasive hemodynamic measurements via right heart catheterization (mean pulmonary arterial pressure (mPAP), systolic- (PAPsys) and diastolic pulmonary arterial pressure (PAPdia), pulmonary arterial wedge pressure (PAWP), a-wave, v-wave, pulmonary vascular resistance (PVR), transpulmonary pressure gradient (TPG), cardiac index (CI), stroke volume index (SVI)). mPAP and PAWP at baseline were neither associated with procedural success, immediate reduction of MR, nor residual MR after 6 months of follow-up. The composite outcome (All-cause mortality (ACM) and/or heart failure induced rehospitalization (HFH)) and HFH differed significantly after M-TEER when stratified according to mPAP, PAWP, PAPdia, a-wave and v-wave. ACM was not associated with the afore mentioned parameters. Neither PVR, TPG, CI nor SVI were associated with the composite outcome and HFH, respectively. In multivariable analyses, PAWP was independently associated with the composite outcome and HFH. PVR and SVI were not associated with outcomes.
PAWP at baseline was significantly and independently associated with HFH and might serve as a valuable parameter for identifying patients at high risk for HFH after M-TEER. ACM and procedural success were not affected by pulmonary arterial pressure before M-TEER. We suggest that the post-capillary component of PH serves as the driving force behind the risk of HFH.
关于二尖瓣反流(MR)患者在接受经导管二尖瓣缘对缘修复术(M-TEER)时,有创测定的血流动力学参数与手术成功率及预后之间关联的数据有限。
我们纳入了239例症状性2+级及以上MR患者,他们接受了M-TEER。所有患者均通过右心导管检查进行了广泛的介入前有创血流动力学测量(平均肺动脉压(mPAP)、收缩期肺动脉压(PAPsys)和舒张期肺动脉压(PAPdia)、肺动脉楔压(PAWP)、a波、v波、肺血管阻力(PVR)、跨肺压梯度(TPG)、心脏指数(CI)、每搏量指数(SVI))。基线时的mPAP和PAWP与手术成功率、MR的即刻降低以及随访6个月后的残余MR均无关联。根据mPAP、PAWP、PAPdia、a波和v波进行分层后,M-TEER后的复合结局(全因死亡率(ACM)和/或心力衰竭导致的再次住院(HFH))以及HFH有显著差异。ACM与上述参数无关。PVR、TPG、CI和SVI分别与复合结局和HFH均无关联。在多变量分析中,PAWP与复合结局和HFH独立相关。PVR和SVI与结局无关。
基线时的PAWP与HFH显著且独立相关,可能是识别M-TEER后HFH高危患者的一个有价值参数。ACM和手术成功率不受M-TEER前肺动脉压的影响。我们认为,PH的毛细血管后成分是HFH风险背后的驱动力。