Houston Methodist DeBakey Heart and Vascular Center Houston TX.
Department of Cardiovascular Surgery Houston Methodist Hospital Houston TX.
J Am Heart Assoc. 2024 Apr 16;13(8):e033510. doi: 10.1161/JAHA.123.033510. Epub 2024 Apr 3.
Pulmonary hypertension (PH) and secondary mitral regurgitation (MR) are associated with adverse outcomes after mitral transcatheter edge-to-edge repair. We aim to study the prognostic value of invasively measured right ventricular afterload in patients undergoing mitral transcatheter edge-to-edge repair.
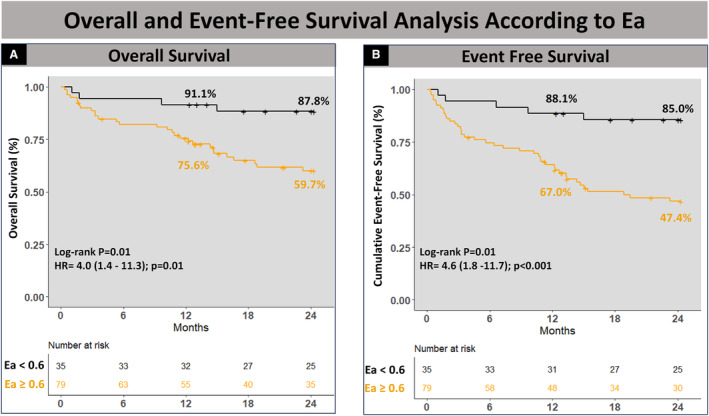
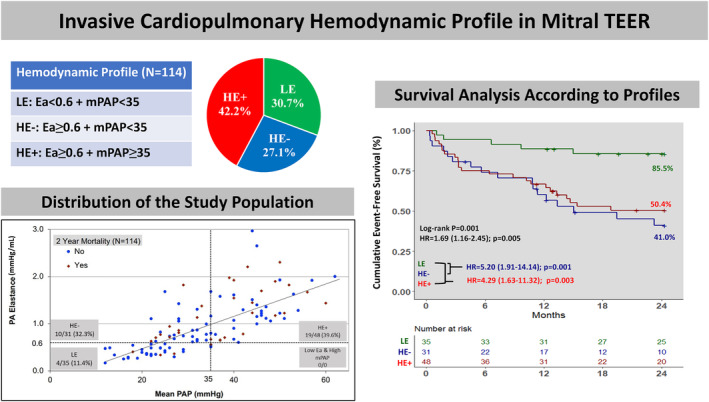
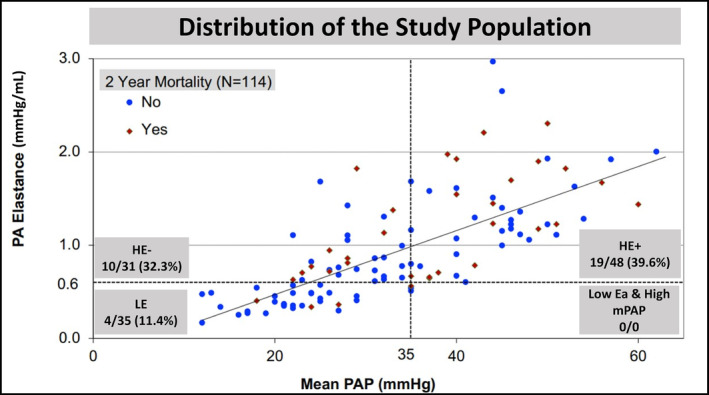
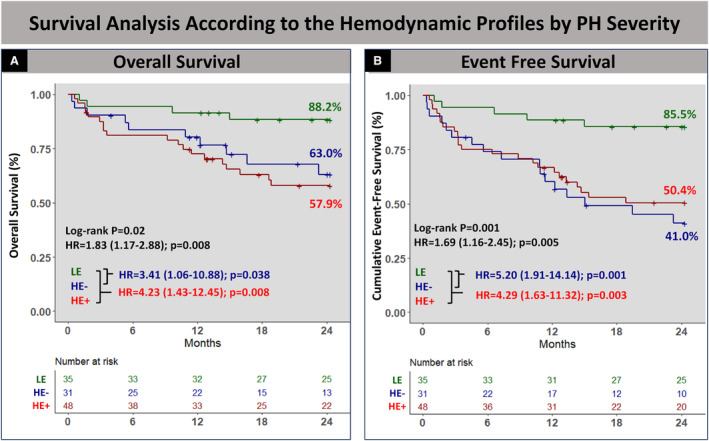
We identified patients who underwent right heart catheterization ≤1 month before transcatheter edge-to-edge repair. The end points were all-cause mortality and a composite of mortality and heart failure hospitalization at 2 years. Using the receiver operating characteristic curve-derived threshold of 0.6 for pulmonary effective arterial elastance ([Ea], pulmonary artery systolic pressure/stroke volume), patients were stratified into 3 profiles based on PH severity (low elastance [HE]: Ea <0.6/mean pulmonary artery pressure (mPAP)) <35; High Elastance with No/Mild PH (HE-): Ea ≥0.6/mPAP <35; and HE with Moderate/Severe PH (HE+): Ea ≥0.6/mPAP ≥35) and MR pathogenesis (Primary MR [PMR])/low elastance, PMR/HE, and secondary MR). The association between this classification and clinical outcomes was examined using Cox regression. Among 114 patients included, 50.9% had PMR. Mean±SD age was 74.7±10.6 years. Patients with Ea ≥0.6 were more likely to have diabetes, atrial fibrillation, New York Heart Association III/IV status, and secondary MR (all <0.05). Overall, 2-year cumulative survival was 71.1% and was lower in patients with secondary MR and mPAP ≥35. Compared with patients with low elastance, cumulative 2-year event-free survival was significantly lower in HE- and HE+ patients (85.5% versus 50.4% versus 41.0%, respectively, =0.001). Also, cumulative 2-year event-free survival was significantly higher in patients with PMR/low elastance when compared with PMR/HE and patients with secondary mitral regurgitation (85.5% versus 55.5% versus 46.1%, respectively, =0.005).
Assessment of the preprocedural cardiopulmonary profile based on mPAP, MR pathogenesis, and Ea guides patient selection by identifying hemodynamic features that indicate likely benefit from mitral-transcatheter edge-to-edge repair in PH or lack thereof.
肺动脉高压(PH)和继发性二尖瓣反流(MR)与二尖瓣经导管缘对缘修复术后的不良结局相关。我们旨在研究经导管二尖瓣缘对缘修复术前测量的右心室后负荷对患者的预后价值。
我们确定了在经导管二尖瓣缘对缘修复术前 1 个月内行右心导管检查的患者。终点为全因死亡率和 2 年时死亡率和心力衰竭住院的复合终点。根据肺动脉有效动脉弹性([Ea],肺动脉收缩压/心排量)的受试者工作特征曲线得出的 0.6 截断值,根据 PH 严重程度(低弹性[HE]:Ea<0.6/平均肺动脉压(mPAP)<35;高弹性无/轻度 PH(HE-):Ea≥0.6/mPAP<35;高弹性伴中度/重度 PH(HE+):Ea≥0.6/mPAP≥35)和 MR 发病机制(原发性 MR [PMR])/低弹性、PMR/HE 和继发性 MR 对患者进行分层。使用 Cox 回归分析这种分类与临床结局之间的关系。在 114 例患者中,50.9%为 PMR。平均年龄±标准差为 74.7±10.6 岁。Ea≥0.6 的患者更可能患有糖尿病、心房颤动、纽约心脏协会 III/IV 级和继发性 MR(均<0.05)。总体而言,2 年累积生存率为 71.1%,继发性 MR 和 mPAP≥35 的患者生存率较低。与低弹性患者相比,HE-和 HE+患者的 2 年累积无事件生存率显著降低(分别为 85.5%、50.4%和 41.0%,=0.001)。此外,与 PMR/HE 和继发性二尖瓣反流患者相比,PMR/低弹性患者的 2 年累积无事件生存率显著更高(分别为 85.5%、55.5%和 46.1%,=0.005)。
根据 mPAP、MR 发病机制和 Ea 评估术前心肺特征,可通过识别可能从 PH 或不存在 PH 的经导管二尖瓣缘对缘修复中获益的血流动力学特征来指导患者选择。