Suelo-Calanao Rona Lee, D'Alessio Andrea, Hutton Sandra, Krasopoulos George, Muppiri Vijayakumar, Cartwright Carly, Parvez Ahmed, Nikolaidis Nicolas, Loubani Mahmoud
Castle Hill Hospital, Hull University Teaching Hospital, Hull, United Kingdom.
Oxford University Hospital, Oxford, United Kingdom.
Interdiscip Cardiovasc Thorac Surg. 2024 May 2;38(5). doi: 10.1093/icvts/ivae056.
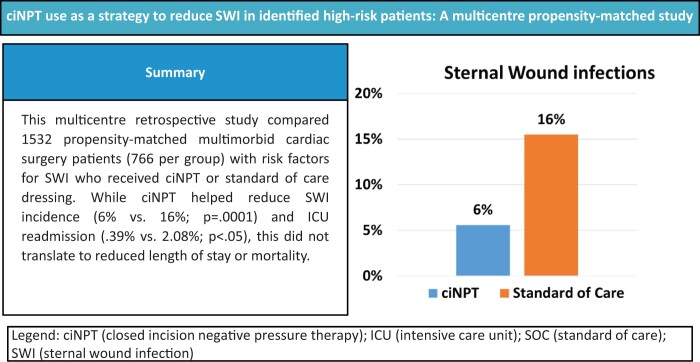
The premise of this retrospective study was to evaluate the intraoperative use of closed-incision negative pressure therapy (ciNPT) to help reduce the incidence of postoperative sternal wound infections in multimorbid patients with an elevated risk of developing a sternal wound infection post cardiac surgery versus a cohort that received standard-of-care dressings.
Data for all adult patients were collected from each cardiothoracic surgery unit across 3 hospitals in the United Kingdom. High-risk patients had 2 or more recognized risk factors. Fisher's exact test (two-tailed) and unpaired t-test were used to help analyse categorical and continuous data. Propensity matching was performed to compare the 2 groups.
A total of 5,288 patients who had cardiac surgery were included. Propensity matching led to 766 matched cases. There were significantly fewer sternal wound infections in the ciNPT group [43 (5.6%) vs 119 (15.5%) cases; P = 0.0001], as well as fewer deep sternal wound infections [14 (1.8%) vs 31 (4.0%) cases; P = 0.0149] and superficial sternal wound infections [29 (3.8%) vs 88 (11.4%) cases; P = 0.0001]. A higher mean length of stay in the ciNPT group was statistically significant (11.23 ± 13 vs 9.66 ± 10 days; P = 0.0083) as was a significantly higher mean logistic European System for Cardiac Operative Risk Evaluation (EuroSCORE) (11.143 ± 13 vs 8.094 ± 11; P = 0.0001). A statistically significant higher readmission to the intensive care unit due to sternal wound infection was noted for the controls [16 (2.08%) vs 3 (0.39%) readmissions; P = 0.0042].
The ciNPT appears to be an effective intervention to help reduce the incidence of sternal wound infection in high-risk individuals undergoing cardiac surgery.
本回顾性研究的前提是评估闭合切口负压疗法(ciNPT)在术中的应用,以帮助降低心脏手术后胸骨伤口感染风险升高的多病患者术后胸骨伤口感染的发生率,并与接受标准护理敷料的队列进行比较。
收集了英国3家医院各心胸外科单元所有成年患者的数据。高危患者有2个或更多公认的风险因素。采用Fisher精确检验(双侧)和非配对t检验来分析分类数据和连续数据。进行倾向匹配以比较两组。
共纳入5288例接受心脏手术的患者。倾向匹配产生了766对匹配病例。ciNPT组的胸骨伤口感染明显较少[43例(5.6%)对119例(15.5%);P = 0.0001],深部胸骨伤口感染也较少[14例(1.8%)对31例(4.0%);P = 0.0149],浅表胸骨伤口感染也较少[29例(3.8%)对88例(11.4%);P = 0.0001]。ciNPT组的平均住院时间显著更长(11.23±13天对9.66±10天;P = 0.0083),平均逻辑欧洲心脏手术风险评估系统(EuroSCORE)也显著更高(11.143±13对8.094±11;P = 0.0001)。对照组因胸骨伤口感染再次入住重症监护病房的比例在统计学上显著更高[16例(2.08%)对3例(0.39%)再入院;P = 0.0042]。
ciNPT似乎是一种有效的干预措施,有助于降低心脏手术高危患者胸骨伤口感染的发生率。