Paediatric Dentistry, Oral Health Sciences, ELOHA (Equal Lifelong Oral Health for All) research group, Ghent University Hospital, Ghent, Belgium.
Department of Reconstructive Dentistry and Oral Biology, Oral Health Sciences, Ghent University Hospital, Ghent, Belgium.
BMC Oral Health. 2024 Apr 10;24(1):437. doi: 10.1186/s12903-024-04132-w.
The trial aimed to compare the clinical performance and radiographic success of ACTIVA BioACTIVE versus Compomer in restoring class-II cavities of primary molars.
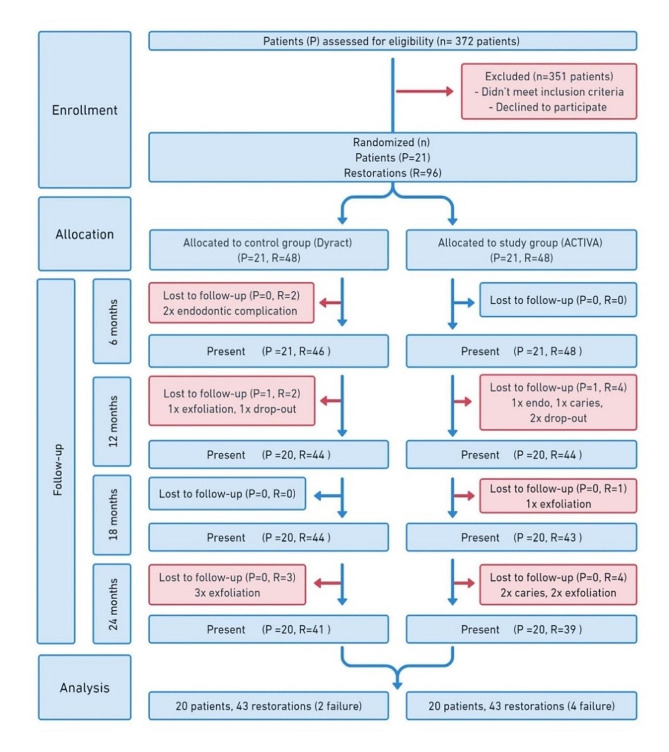
A non-inferior split-mouth design was considered. A pre-calculated sample size of 96 molars (48 per group) with class-2 cavities of twenty-one children whose ages ranged from 5 to 10 years were randomly included in the trial. Pre-operative Plaque Index (PI), DMFT/dmft scores and the time required to fill the cavity were recorded. Over 24 months, the teeth were clinically evaluated every six months and radiographically every 12 months by two calibrated and blinded evaluators using the United States public health service (USPHS)-Ryge criteria. The two-sided 95% confidence interval (CI) for the difference in success rate was considered to assess non-inferiority, and the margin was set at -18%. The linear mixed model and Firth's logistic regression model were used for data analysis (P < 0.05).
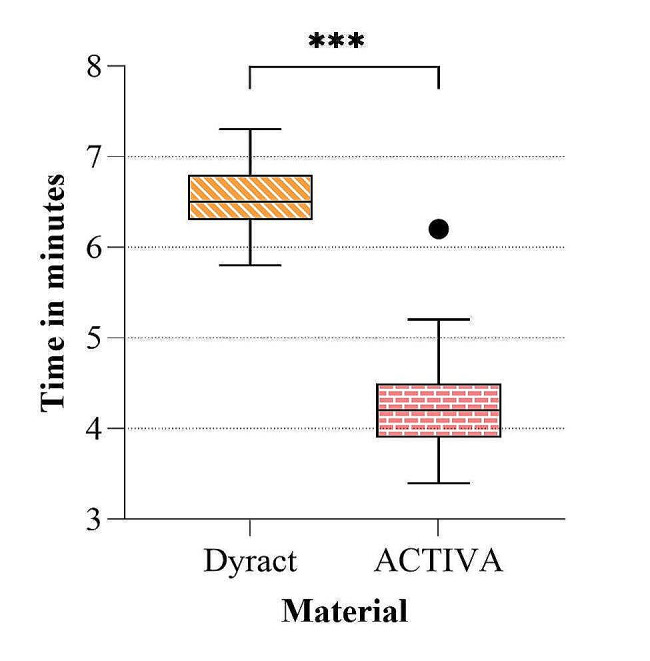
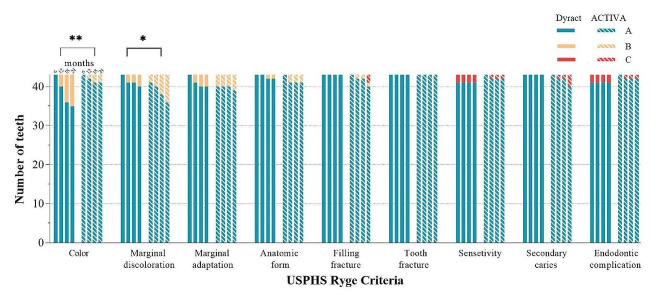
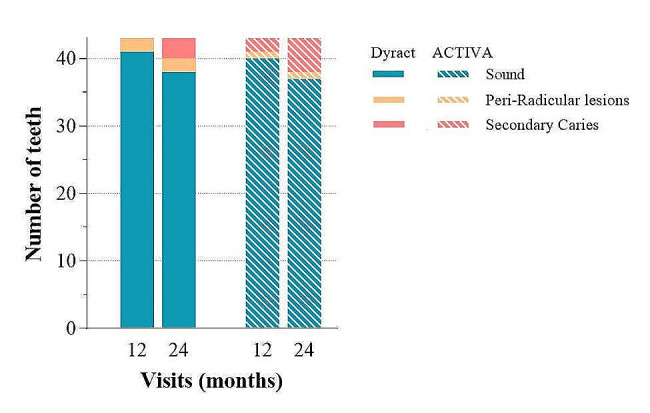
After 24 months, 86 teeth (43 per group) were evaluated. The mean PI score was 1.1(± 0.9), while DMFT/dmft was 0.35 (± 0.74) and 6.55 (± 2.25) respectively. The clinical and radiographic success rate of Dyract vs. ACTIVA was 95.3% and 88.3% vs. 93% and 86%, respectively. The two-sided 95% CI for the difference in success rate (-2.3%) was - 3.2 to 1.3% and didn't reach the predetermined margin of -18% which had been anticipated as the non-inferiority margin. Clinically, ACTIVA had a significantly better colour match (P = 0.002) but worse marginal discolouration (P = 0.0143). There were no significant differences regarding other clinical or radiographic criteria (P > 0.05). ACTIVA took significantly less placement time than Dyract, with a mean difference of 2.37 (± 0.63) minutes (P < 0.001).
The performance of ACTIVA was not inferior to Dyract and both materials had a comparable high clinical and radiographic performance in children with high-caries experience. ACTIVA had a significantly better colour match but more marginal discolouration. It took significantly less time to be placed in the oral cavity.
The study was registered at ClinicalTrials.gov on 4 May 2018 (#NCT03516838).
本试验旨在比较 ACTIVA BioACTIVE 与 Compomer 修复乳磨牙Ⅱ类洞的临床性能和放射学成功率。
采用非劣效性劈裂口设计。将 21 名年龄在 5 至 10 岁之间的儿童的 96 颗(每组 48 颗)Ⅱ类窝洞的磨牙按预计算的样本量随机纳入试验。记录术前菌斑指数(PI)、DMFT/dmft 评分和填充窝洞所需的时间。在 24 个月的时间里,每 6 个月进行一次临床评估,每 12 个月进行一次放射学评估,由 2 名经过校准和盲法评估的评估员使用美国公共卫生服务(USPHS)-Ryge 标准进行评估。采用双侧 95%置信区间(CI)评估成功率差异,以评估非劣效性,边际设定为-18%。采用线性混合模型和 Firth 逻辑回归模型进行数据分析(P<0.05)。
24 个月后,共评估了 86 颗牙齿(每组 43 颗)。平均 PI 评分为 1.1(±0.9),DMFT/dmft 分别为 0.35(±0.74)和 6.55(±2.25)。Dyract 与 ACTIVA 的临床和放射学成功率分别为 95.3%和 88.3%与 93%和 86%。成功率差异的双侧 95%CI(-2.3%)为-3.2 至 1.3%,未达到预期的非劣效性边际-18%。临床上,ACTIVA 的颜色匹配明显更好(P=0.002),但边缘变色较差(P=0.0143)。其他临床或放射学标准无显著差异(P>0.05)。ACTIVA 的放置时间明显短于 Dyract,平均差异为 2.37(±0.63)分钟(P<0.001)。
ACTIVA 的性能不劣于 Dyract,在高龋经验儿童中,两种材料均具有较高的临床和放射学性能。ACTIVA 的颜色匹配明显更好,但边缘变色更多。它在口腔中放置的时间明显更短。
该研究于 2018 年 5 月 4 日在 ClinicalTrials.gov 注册(#NCT03516838)。