Tsur Eyal, Blumenfeld Philip, Rottenberg Yakir, Nechushtan Hovav, Arnon Johnathan, Wald Ori, Izhar Uzi, Pfeffer Raphael, Krakow Aron, Wygoda Marc, Popovtzer Aron, Michaeli Tal Falick
Department of Military Medicine, "Tzameret", and Medical Corps, Israel Defense Forces, Ramat Gan, Israel.
Department of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel.
Transl Lung Cancer Res. 2024 Mar 29;13(3):465-474. doi: 10.21037/tlcr-23-802. Epub 2024 Mar 22.
Stereotactic body radiation therapy (SBRT) is often delivered in patients with oligometastatic disease (OMD). However, the specific subset of patients with polymetastatic non-small cell lung cancer (NSCLC) on novel systemic therapies who develop induced oligopersistant disease (OpersisD) or oligoprogressive disease (OprogD), as defined by the European Organisation for Research and Treatment of Cancer (EORTC) OMD classification, has not been well described. This study explores the outcomes of patients treated with this strategy.
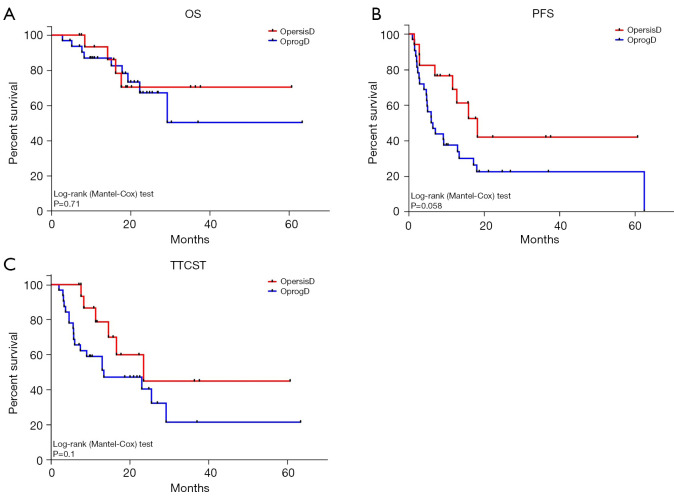
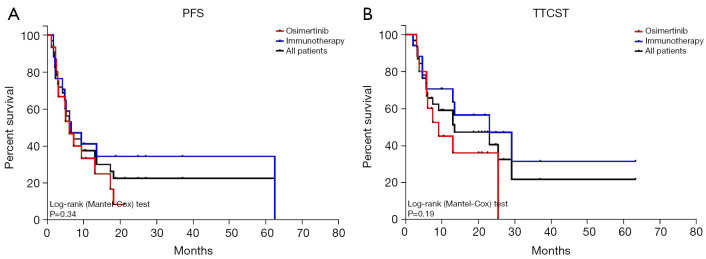
Patients with stage IV NSCLC being treated with osimertinib or immune checkpoint inhibitors (ICIs) who received extracranial SBRT for OpersisD or OprogD were identified in our retrospective analysis. Outcomes reported include progression-free survival (PFS), time to change of systemic treatment (TTCST), overall survival (OS), local control (LC) and treatment-related toxicity.
Forty-nine patients received SBRT for OpersisD (34.7%) or OprogD (65.3%) at a median of 5.8 and 15.3 months after start of systemic therapy, respectively. 55.1% received concurrent osimertinib and 44.9% received ICI. Seventy-seven extracranial lesions were treated with various fractionation schemas. At a median of 18.8 months follow-up from first SBRT, LC was achieved in 92.2% of total lesions treated (71). The 1-year OS was 91.7% for OpersisD and 83.3% for OprogD. OpersisD compared to OprogD had a longer median PFS (18.3 6.1 months) and longer median TTCST (23.6 13.5 months), median OS was not reached for either cohort. On multivariate analysis, patients treated with osimertinib had shorter PFS (HR: 2.20; 95% CI: 1.01-4.82; P=0.048) and shorter TTCST (HR: 2.83; 95% CI: 1.09-7.33; P=0.032). One patient (2%) experienced grade 3 pneumonitis after SBRT, and no grade 4-5 toxicities were reported with SBRT treatment.
This study indicates that SBRT for OpersisD or OprogD in Stage IV NSCLC patients on osimertinib or ICIs is safe, very well tolerated, and may prolong the time before needing a shift in systemic therapy. Further prospective research is needed to validate and expand upon these findings.
立体定向体部放射治疗(SBRT)常用于寡转移疾病(OMD)患者。然而,对于接受新型全身治疗的多转移非小细胞肺癌(NSCLC)患者中,按照欧洲癌症研究与治疗组织(EORTC)OMD分类定义发生诱导性寡持续性疾病(OpersisD)或寡进展性疾病(OprogD)的特定亚组,目前尚未得到充分描述。本研究探讨了采用该策略治疗的患者的预后情况。
在我们的回顾性分析中,确定了接受奥希替尼或免疫检查点抑制剂(ICI)治疗的IV期NSCLC患者,这些患者因OpersisD或OprogD接受了颅外SBRT。报告的预后指标包括无进展生存期(PFS)、全身治疗改变时间(TTCST)、总生存期(OS)、局部控制率(LC)和治疗相关毒性。
49例患者分别在全身治疗开始后的中位5.8个月和15.3个月因OpersisD(34.7%)或OprogD(65.3%)接受了SBRT。55.1%的患者同时接受奥希替尼治疗,44.9%的患者接受ICI治疗。77个颅外病灶采用了不同的分割方案进行治疗。从首次SBRT开始的中位随访18.8个月时,92.2%(71个)接受治疗的总病灶实现了局部控制。OpersisD患者的1年总生存率为91.7%,OprogD患者为83.3%。与OprogD相比,OpersisD的中位PFS更长(18.3±6.1个月),中位TTCST更长(23.6±13.5个月),两个队列的中位OS均未达到。多因素分析显示,接受奥希替尼治疗的患者PFS较短(HR:2.20;95%CI:1.01 - 4.82;P = 0.048),TTCST较短(HR:2.83;95%CI:1.09 - 7.33;P = 0.032)。1例患者(2%)在SBRT后发生3级肺炎,SBRT治疗未报告4 - 5级毒性反应。
本研究表明,对于接受奥希替尼或ICI治疗的IV期NSCLC患者的OpersisD或OprogD进行SBRT是安全的,耐受性良好,并且可能延长需要改变全身治疗之前的时间。需要进一步的前瞻性研究来验证和扩展这些发现。