Norimatsu Yu, Takemura Nobuyuki, Yoshikawa Kaoru, Ito Kyoji, Inagaki Fuyuki, Mihara Fuminori, Yamada Kazuhiko, Kokudo Norihiro
Hepato-Biliary-Pancreatic Surgery Division, Department of Surgery, National Center for Global Health and Medicine, 1-21-1 Toyama, Shinjuku-ku, Tokyo, 162-8655, Japan.
Surg Case Rep. 2024 Apr 12;10(1):84. doi: 10.1186/s40792-024-01882-1.
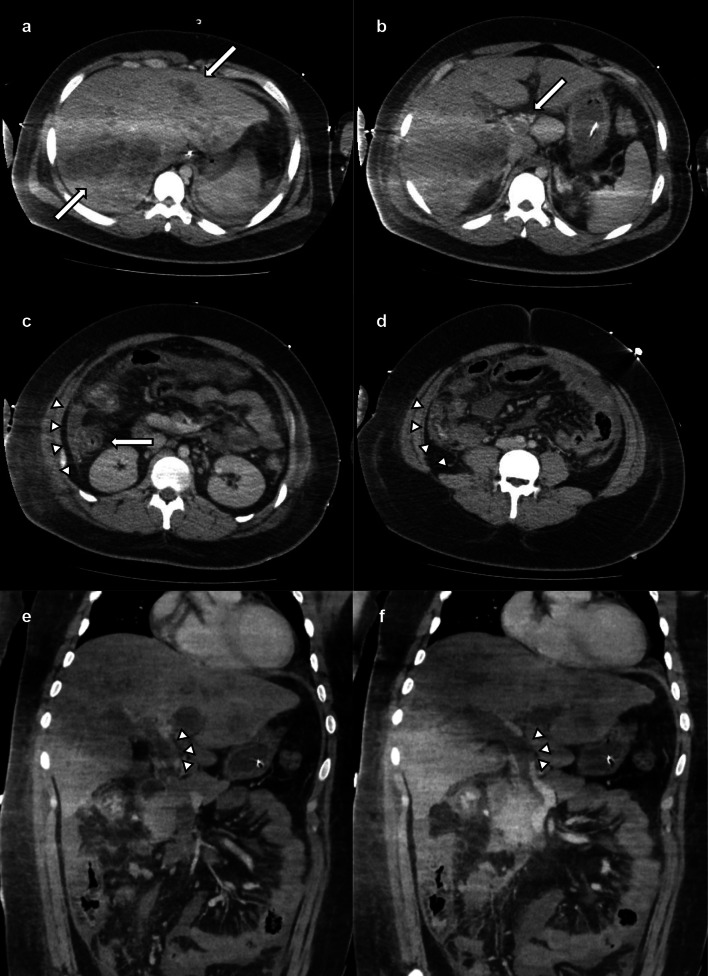
Pylephlebitis, a rare and lethal form of portal venous septic thrombophlebitis, often arises from infections in regions drained by the portal vein. Herein, we report a case of peritonitis with portal vein thrombosis due to acute severe appendicitis, managed with intensive intraperitoneal drainage via open abdominal management (OAM).
A 19-year-old male with severe appendicitis, liver abscesses, and portal vein thrombosis developed septic shock and multi-organ failure. After emergency interventions, the patient was admitted to the intensive care unit. Antibiotic treatment based on cultures revealing multidrug-resistant Escherichia coli and Bacteroides fragilis and anticoagulation therapy (using heparin and edoxaban) was initiated. Despite continuous antibiotic therapy, the laboratory results consistently showed elevated levels of inflammatory markers. On the 13th day, open abdominal irrigation was performed for infection control. Extensive intestinal edema precluded wound closure, necessitating open-abdominal management in the intensive care unit. Anticoagulation therapy was continued, and intra-abdominal washouts were performed every 5 days. On the 34th day, wound closure was achieved using the anterior rectus abdominis sheath turnover method. The patient recovered successfully and was discharged on the 81st day.
Alongside appropriate antibiotic selection, early surgical drainage and OAM are invaluable. This case underscores the potential of anticoagulation therapy in facilitating safe surgical procedures.
门静脉脓毒性血栓性静脉炎是一种罕见且致命的门静脉败血症形式,通常源于门静脉引流区域的感染。在此,我们报告一例因急性重症阑尾炎导致腹膜炎合并门静脉血栓形成的病例,通过开放腹腔管理(OAM)进行强化腹腔引流治疗。
一名19岁男性,患有重症阑尾炎、肝脓肿和门静脉血栓形成,并发感染性休克和多器官功能衰竭。经过紧急干预后,患者被收入重症监护病房。根据培养结果显示多重耐药大肠杆菌和脆弱拟杆菌,开始使用抗生素治疗并进行抗凝治疗(使用肝素和依度沙班)。尽管持续进行抗生素治疗,但实验室结果始终显示炎症标志物水平升高。在第13天,为控制感染进行了开放腹腔冲洗。广泛的肠水肿妨碍了伤口闭合,因此在重症监护病房进行开放腹腔管理。继续进行抗凝治疗,每5天进行一次腹腔冲洗。在第34天,采用腹直肌前鞘翻转法实现了伤口闭合。患者成功康复并于第81天出院。
除了选择合适的抗生素外,早期手术引流和OAM非常重要。该病例强调了抗凝治疗在促进安全手术过程中的潜力。