Division of Vascular Surgery, University of Utah, School of Medicine, Salt Lake City, UT; Department of Population Health Science, University of Utah, School of Medicine, Salt Lake City, UT.
Division of Vascular Surgery, University of Utah, School of Medicine, Salt Lake City, UT.
J Vasc Surg. 2024 Aug;80(2):466-477.e4. doi: 10.1016/j.jvs.2024.03.455. Epub 2024 Apr 10.
Society for Vascular Surgery guidelines recommend revascularization for patients with intermittent claudication (IC) if it can improve patient function and quality of life. However, it is still unclear if patients with IC achieve a significant functional benefit from surgery compared with medical management alone. This study examines the relationship between IC treatment modality (operative vs nonoperative optimal medical management) and patient-reported outcomes for physical function (PROMIS-PF) and satisfaction in social roles and activities (PROMIS-SA).
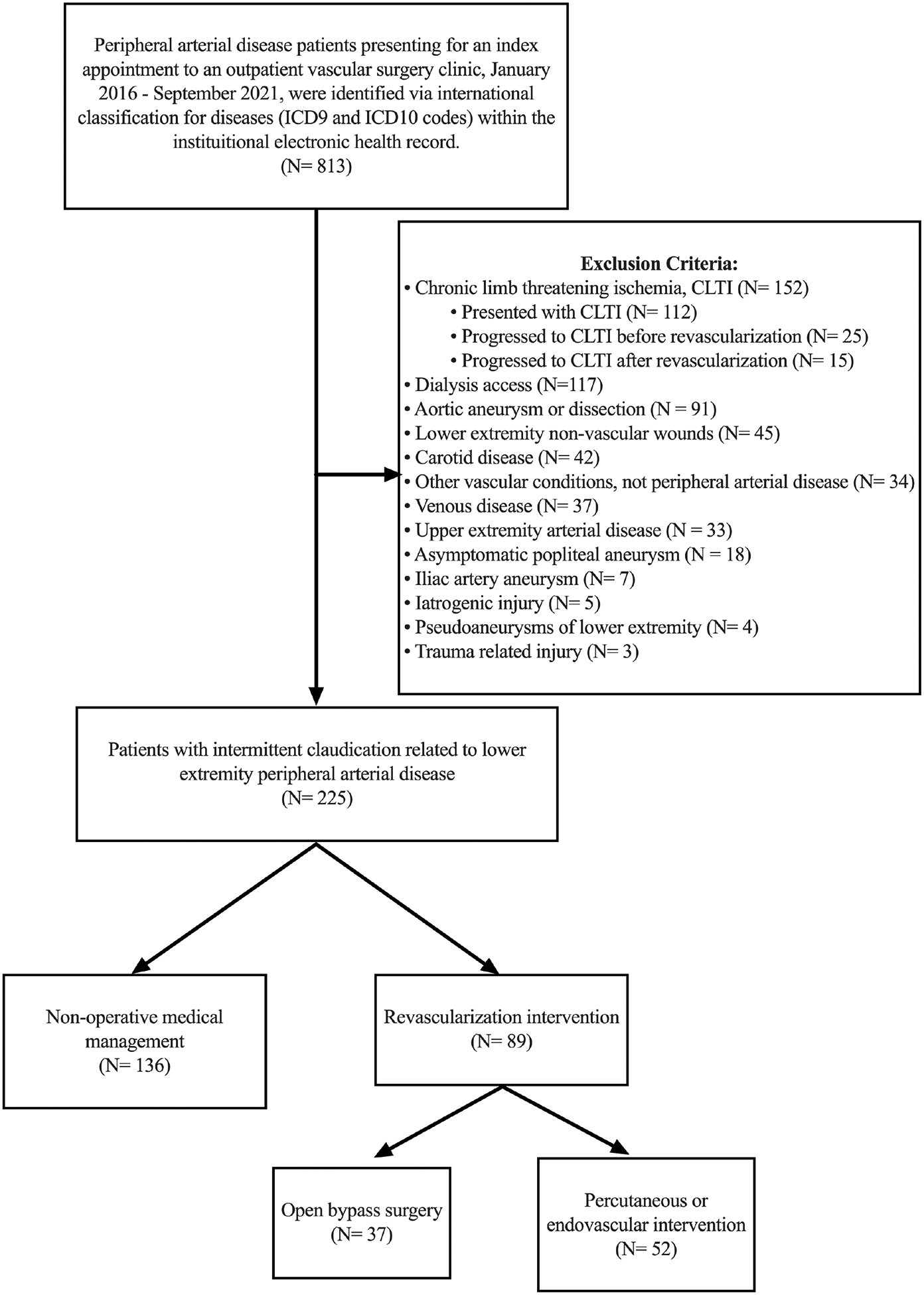
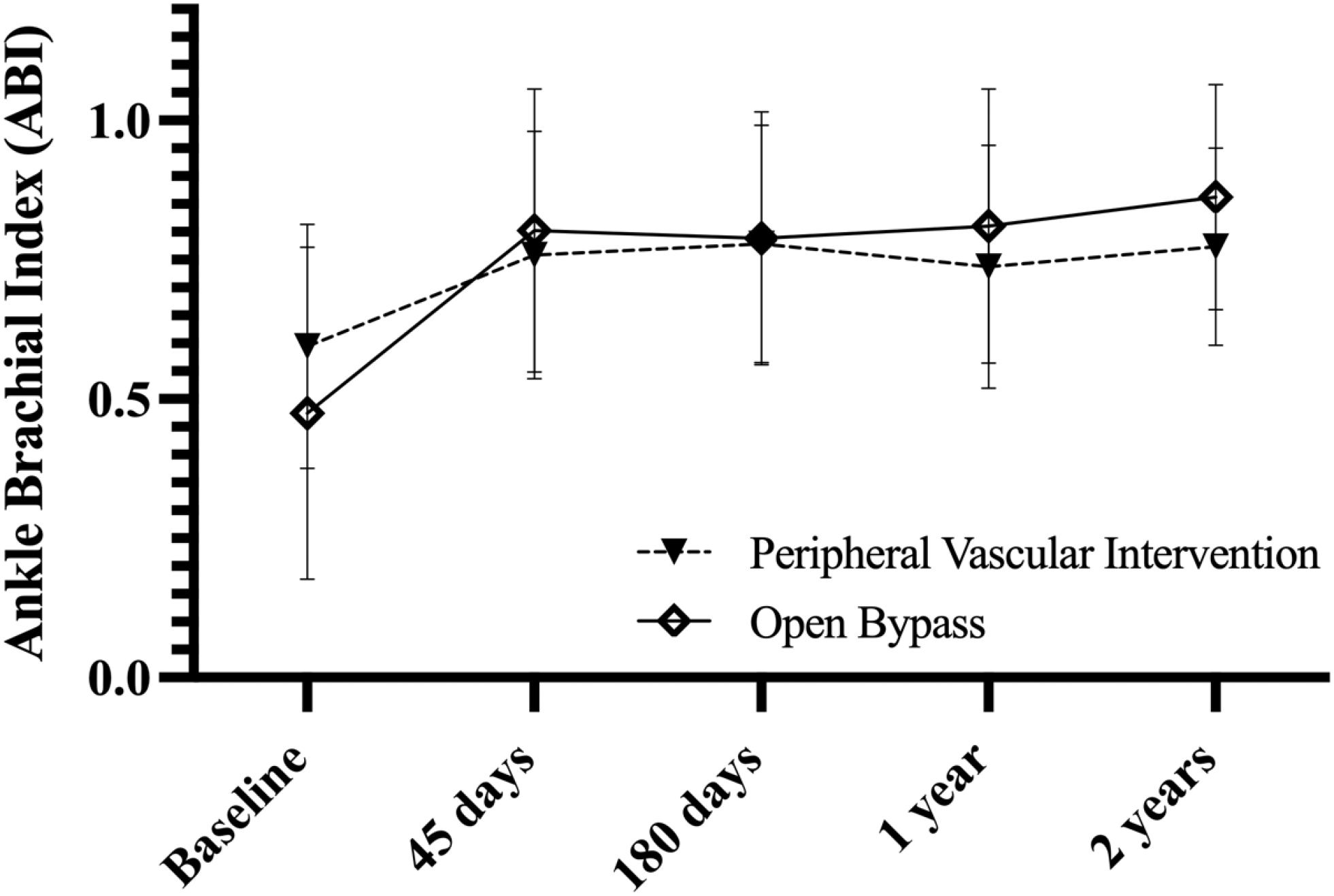
We identified patients with IC who presented for index evaluation in a vascular surgery clinic at an academic medical center between 2016 and 2021. Patients were stratified based on whether they underwent a revascularization procedure during follow-up vs continued nonoperative management with medication and recommended exercise therapy. We used linear mixed-effect models to assess the relationship between treatment modality and PROMIS-PF, PROMIS-SA, and ankle-brachial index (ABI) over time, clustering among repeat patient observations. Models were adjusted for age, sex, diabetes, Charlson Comorbidity Index, Clinical Frailty Score, tobacco use, and index ABI.
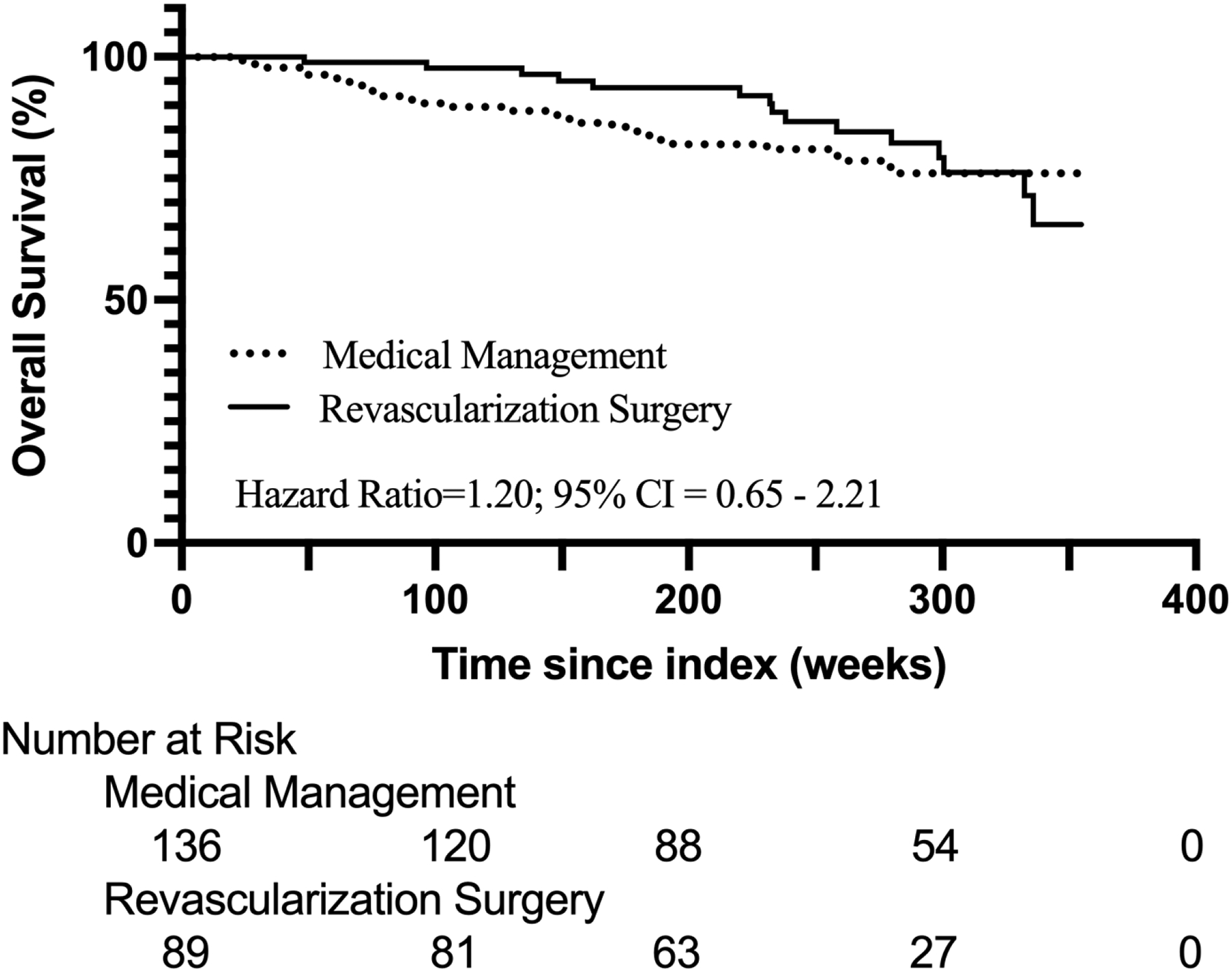
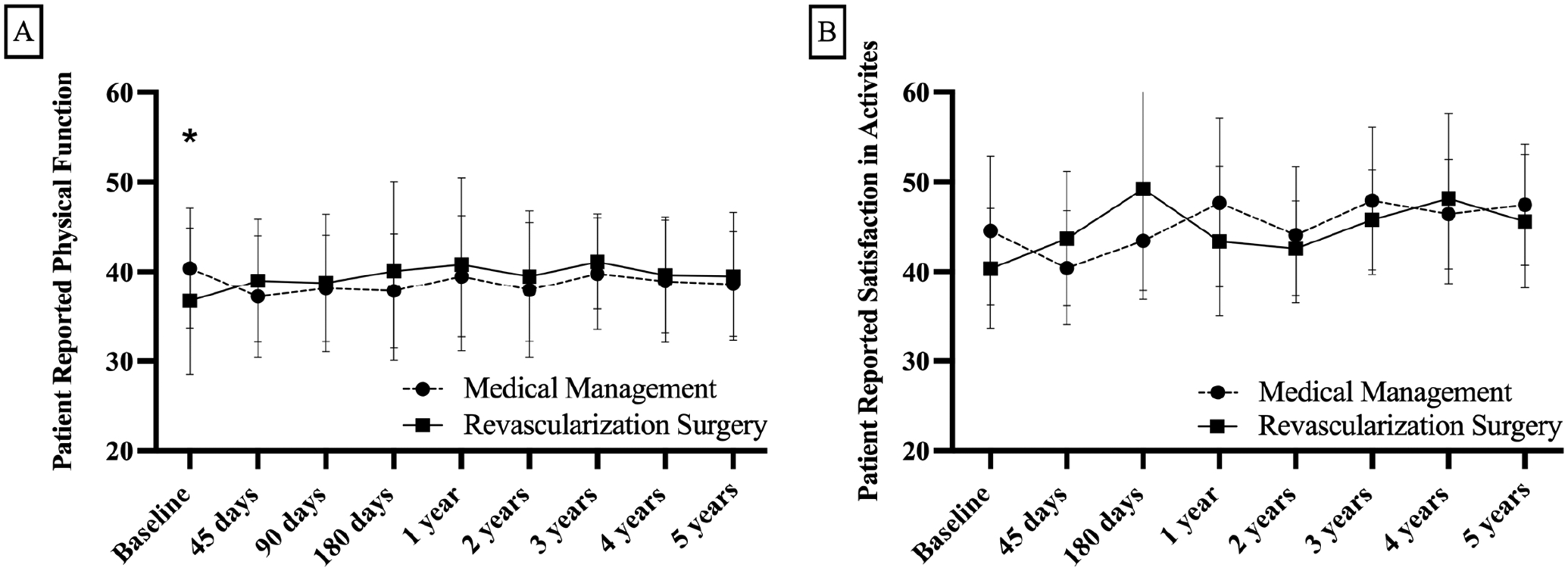
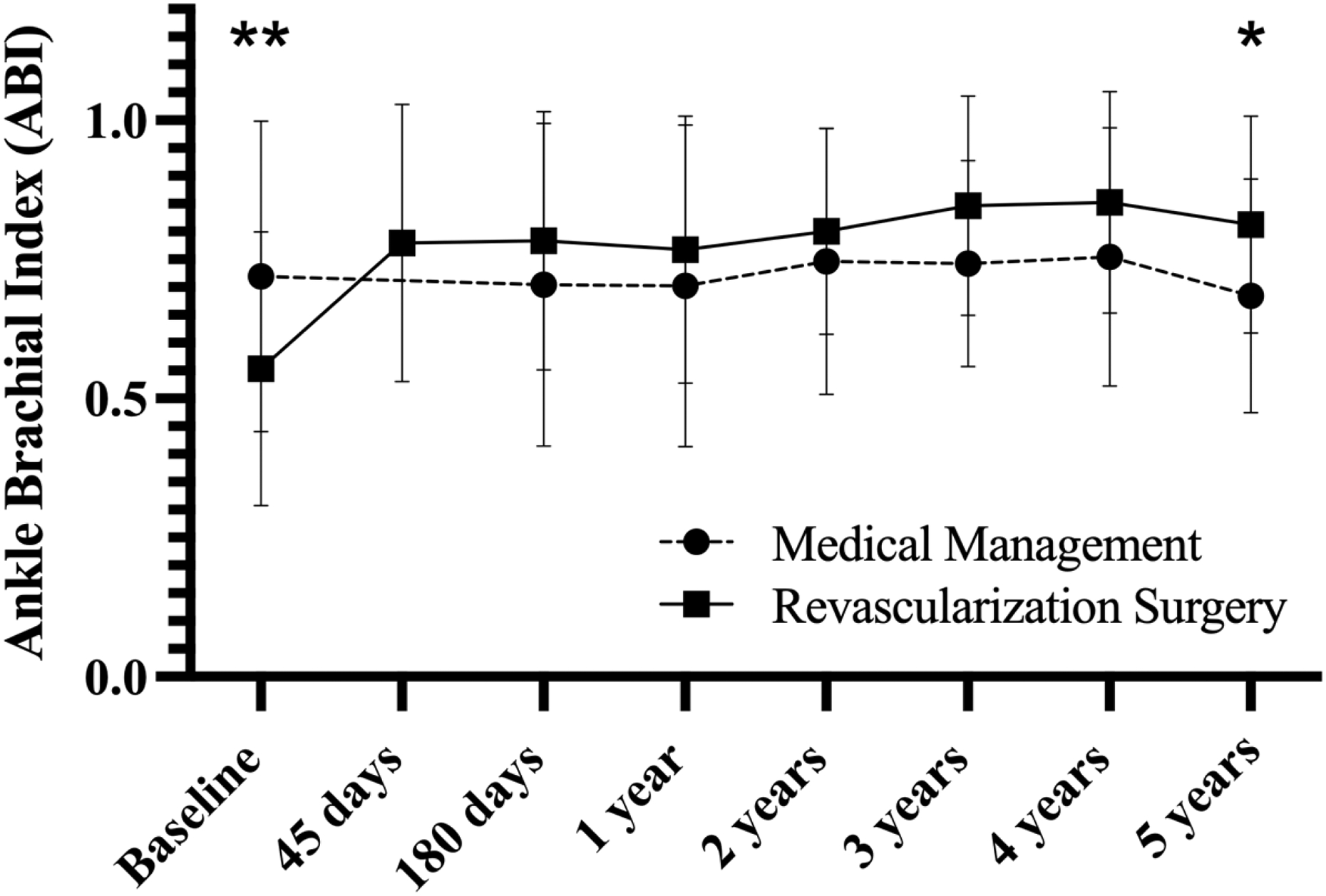
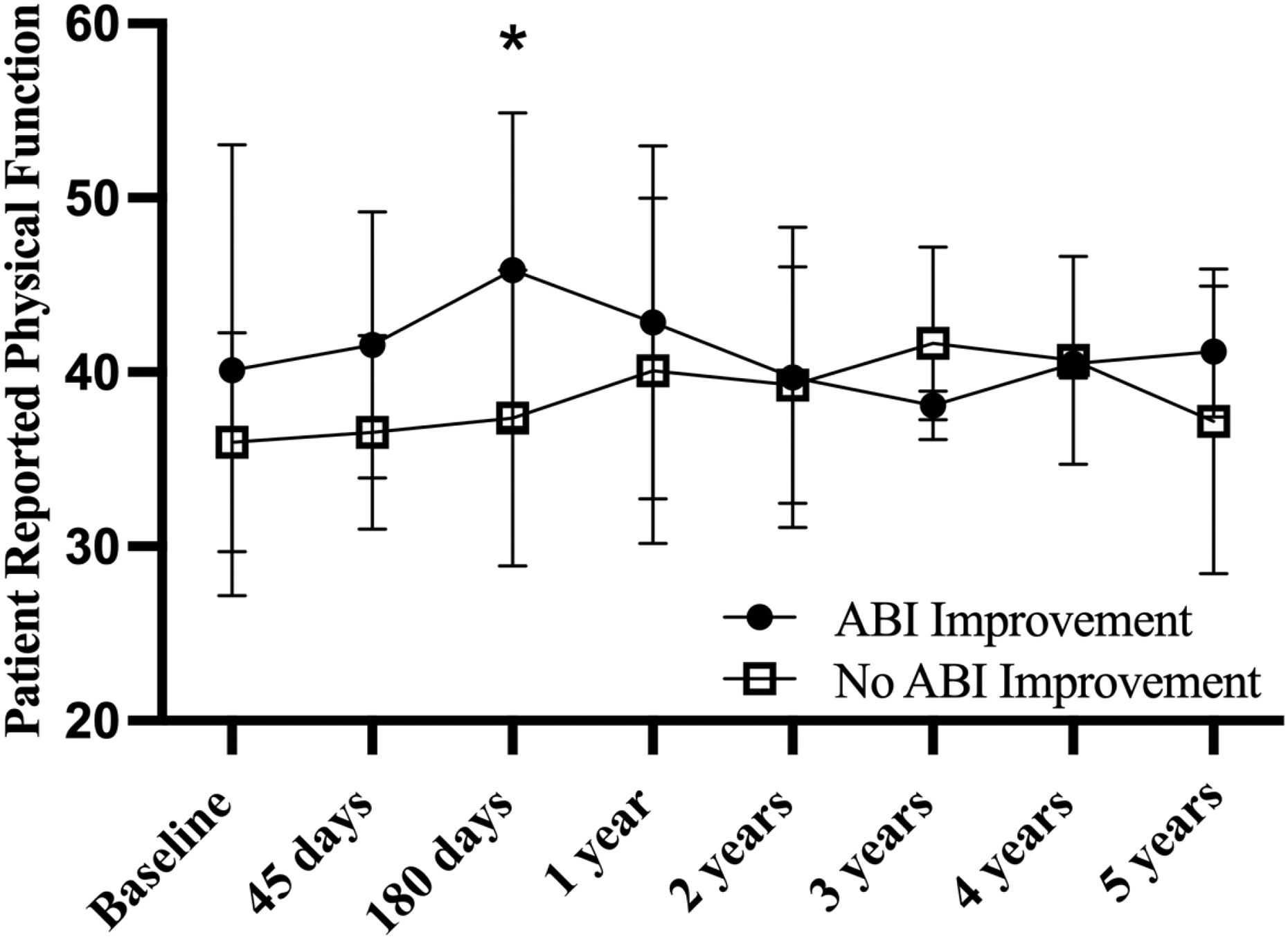
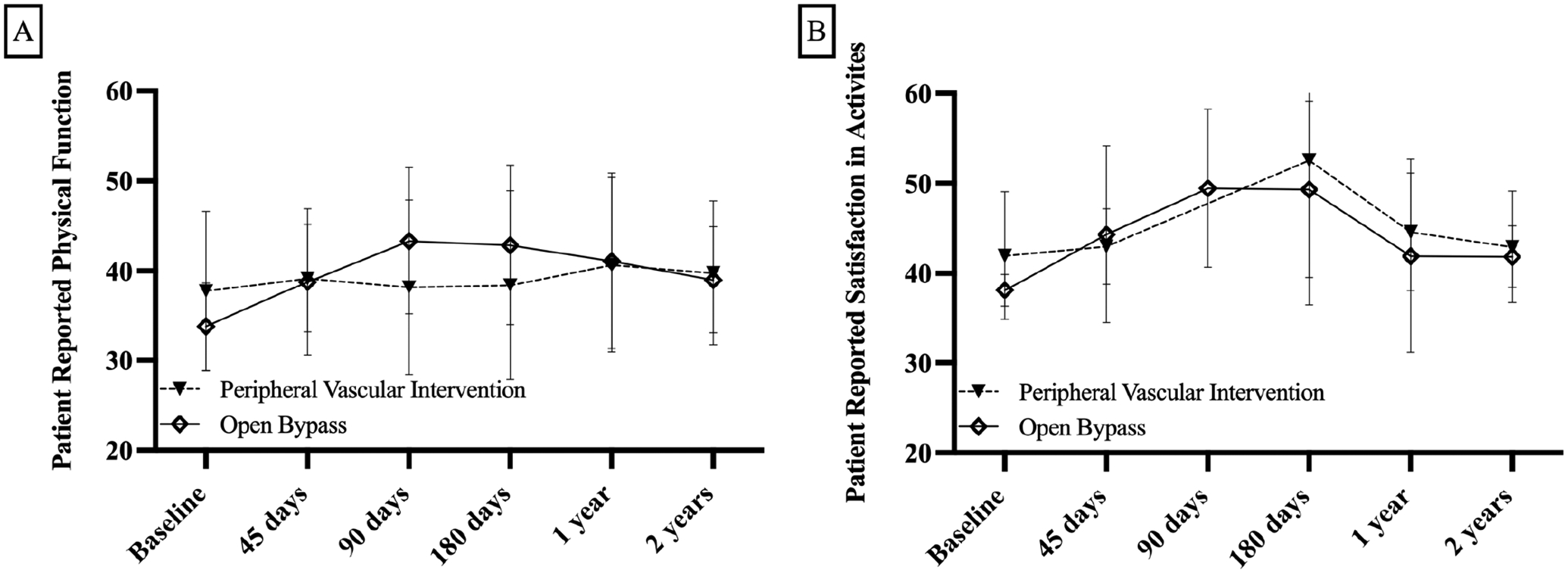
A total of 225 patients with IC were identified, of which 40% (n = 89) underwent revascularization procedures (42% bypass; 58% peripheral vascular intervention) and 60% (n = 136) continued nonoperative management. Patients were followed up to 6.9 years, with an average follow-up of 5.2 ± 1.6 years. Patients who underwent revascularization were more likely to be clinically frail (P = .03), have a lower index ABI (0.55 ± 0.24 vs 0.72 ± 0.28; P < .001), and lower baseline PROMIS-PF score (36.72 ± 8.2 vs 40.40 ± 6.73; P = .01). There were no differences in patient demographics or medications between treatment groups. Examining patient-reported outcome trends over time; there were no significant differences in PROMIS-PF between groups, trends over time, or group differences over time after adjusting for covariates (P = .07, P = .13, and P =.08, respectively). However, all patients with IC significantly increased their PROMIS-SA over time (adjusted P = .019), with patients managed nonoperatively more likely to have an improvement in PROMIS-SA over time than those who underwent revascularization (adjusted P = .045).
Patient-reported outcomes associated with functional status and satisfaction in activities are similar for patients with IC for up to 7 years, irrespective of whether they undergo treatment with revascularization or continue nonoperative management. These findings support conservative long-term management for patients with IC.
血管外科学会指南建议间歇性跛行(IC)患者进行血运重建,如果能改善患者的功能和生活质量。然而,IC 患者是否能从手术中获得显著的功能获益,仍不明确,与单纯药物和推荐的运动疗法相比。本研究检测了 IC 治疗方式(手术与非手术最佳药物治疗)与身体功能(PROMIS-PF)和社会角色及活动满意度(PROMIS-SA)患者报告结局之间的关系。
我们在 2016 年至 2021 年期间,在学术医疗中心的血管外科诊所中,对出现间歇性跛行症状的患者进行了评估。患者根据随访期间是否接受了血运重建手术或继续进行药物治疗和推荐的运动疗法,分为手术和非手术治疗。我们使用线性混合效应模型,在考虑重复患者观察的情况下,评估了治疗方式与 PROMIS-PF、PROMIS-SA 和踝肱指数(ABI)之间的关系。模型调整了年龄、性别、糖尿病、Charlson 合并症指数、临床虚弱评分、吸烟状况和初始 ABI。
共纳入 225 例 IC 患者,40%(n=89)接受了血运重建手术(42%搭桥术;58%外周血管介入术),60%(n=136)继续接受非手术治疗。患者平均随访 5.2±1.6 年,随访时间最长达 6.9 年。接受血运重建的患者更可能处于临床虚弱状态(P=0.03),初始 ABI 更低(0.55±0.24 比 0.72±0.28;P<0.001),基线 PROMIS-PF 评分更低(36.72±8.2 比 40.40±6.73;P=0.01)。两组患者的人口统计学和药物治疗无差异。在评估患者报告结局的趋势时;在调整了协变量后,两组间的 PROMIS-PF 无显著差异(P=0.07),随时间的变化趋势无差异(P=0.13),以及调整后的时间变化差异无差异(P=0.08)。然而,所有 IC 患者的 PROMIS-SA 均随时间显著增加(调整后 P=0.019),与接受血运重建的患者相比,非手术治疗的患者随时间推移更有可能改善 PROMIS-SA(调整后 P=0.045)。
在长达 7 年的时间里,IC 患者的身体功能和活动满意度相关的患者报告结局相似,无论他们接受血运重建治疗还是继续非手术治疗。这些发现支持对 IC 患者进行长期保守治疗。