Aluisio Adam R, Smith-Sreen Joshua, Offorjebe Agatha, Maina Wamutitu, Pirirei Sankei, Kinuthia John, Bukusi David, Waweru Harriet, Bosire Rose, Ojuka Daniel K, Eastment McKenna C, Katz David A, Mello Michael J, Farquhar Carey
Department of Emergency Medicine, Alpert Medical School of Brown University, Providence, USA.
Alpert Medical School of Brown University, Providence, USA.
medRxiv. 2024 Apr 4:2024.04.03.24305277. doi: 10.1101/2024.04.03.24305277.
Persons seeking emergency injury care are often from underserved key populations (KPs) and priority populations (PPs) for HIV programming. While facility-based HIV Testing Services (HTS) in Kenya are effective, emergency department (ED) delivery is limited, despite the potential to reach underserved persons.
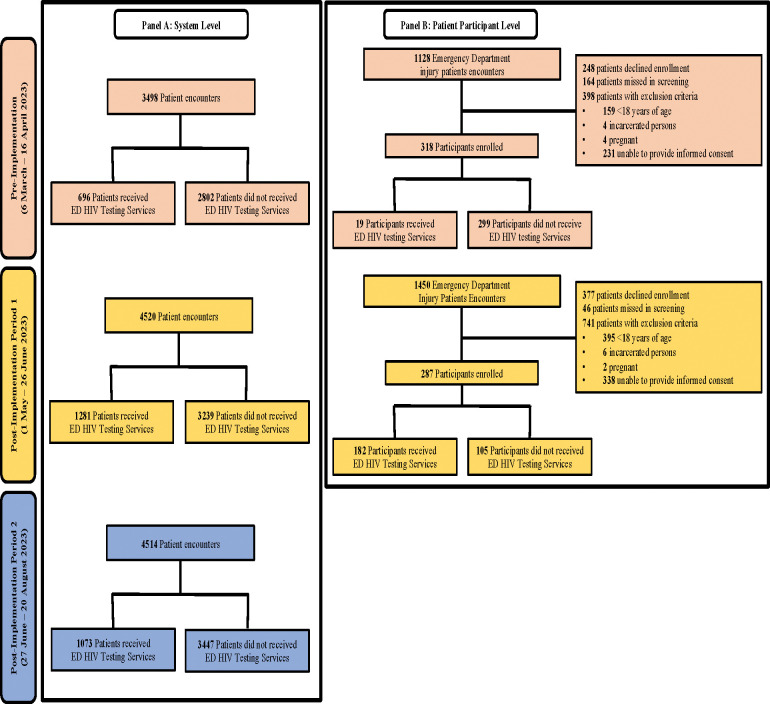
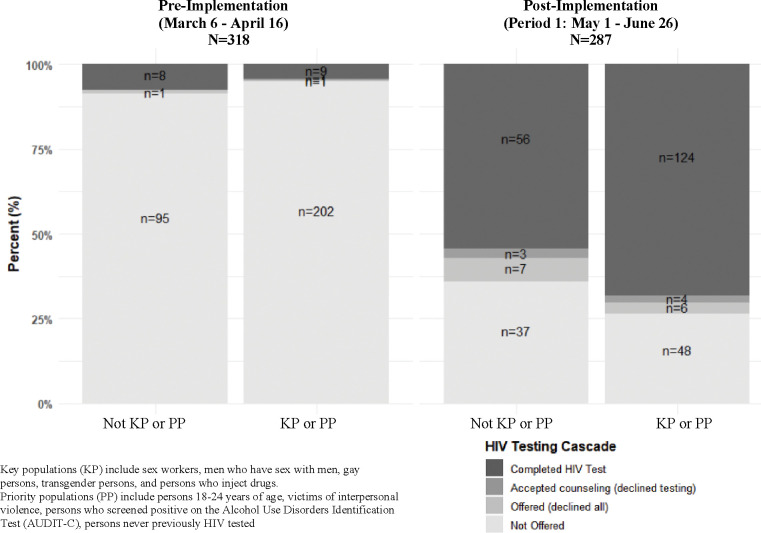
This quasi-experimental prospective study evaluated implementation of the HIV Enhanced Access Testing in Emergency Departments (HEATED) at Kenyatta National Hospital ED in Nairobi, Kenya. The HEATED program was designed using setting specific data and utilizes resource reorganization, services integration and HIV sensitization to promote ED-HTS. KPs included sex workers, gay men, men who have sex with men, transgender persons and persons who inject drugs. PPs included young persons (18-24 years), victims of interpersonal violence, persons with hazardous alcohol use and those never previously HIV tested. Data were obtained from systems-level records, enrolled injured patient participants and healthcare providers. Systems and patient-level data were collected during a pre-implementation period (6 March - 16 April 2023) and post-implementation (period 1, 1 May - 26 June 2023). Additional, systems-level data were collected during a second post-implementation (period 2, 27 June - 20 August 2023). Evaluation analyses were completed across reach, effectiveness, adoption, implementation and maintenance framework domains.
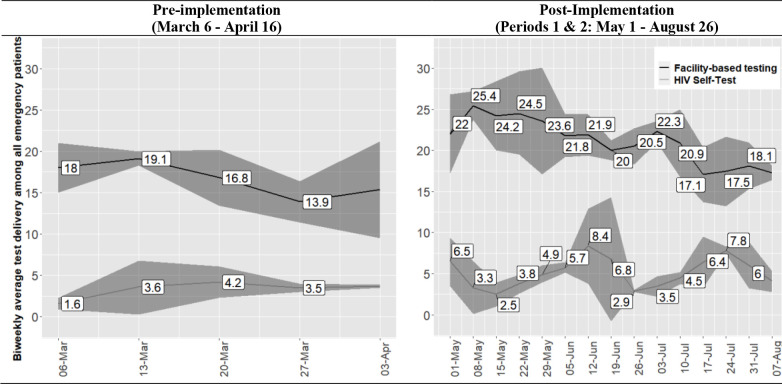
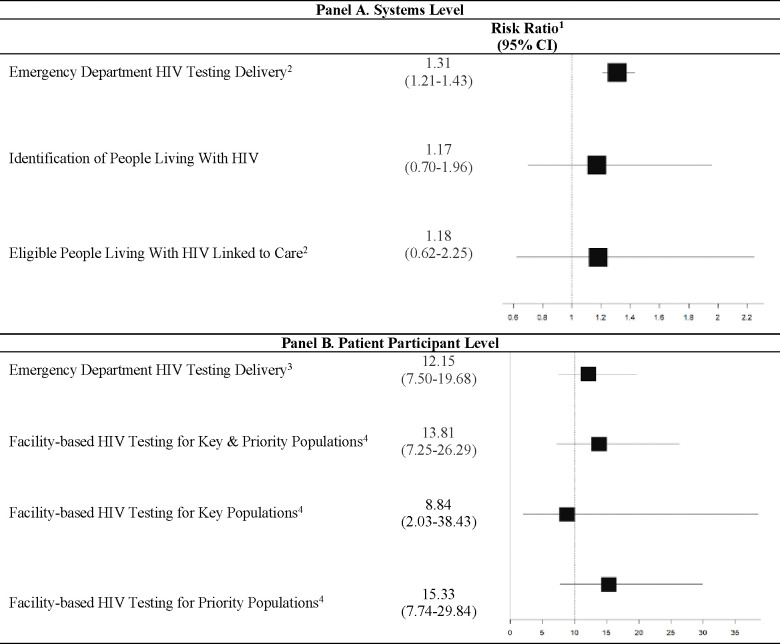
All 151 clinical staff were reached through trainings and sensitizations on the HEATED program. Systems-level ED-HTS increased from 16.7% pre-implementation to 23.0% post-implementation periods 1 and 2 (RR=1.31, 95% CI:1.21-1.43; p<0.001) with a 62.9% relative increase in HIV self-test kit provision. Among 605 patient participants, facilities-based HTS increased from 5.7% pre-implementation to 62.3% post-implementation period 1 (RR=11.2, 95%CI:6.9-18.1; p<0.001). There were 440 (72.7%) patient participants identified as KPs (5.6%) and/or PPs (65.3%). For enrolled KPs/PPs, HTS increased from 4.6% pre-implementation to 72.3% post-implementation period 1 (RR=13.8, 95%CI:5.5-28.7, p<0.001). Systems and participant level data demonstrated successful adoption and implementation of the HEATED program. Through 16-weeks post-implementation a significant increase in ED-HTS delivery was maintained as compared to pre-implementation.
The HEATED program increased ED-HTS and augmented delivery to KPs/PPs, suggesting that broader implementation could improve HIV services for underserved persons, already in contact with health systems.
寻求紧急创伤护理的人群往往来自艾滋病规划中服务不足的重点人群(KPs)和优先人群(PPs)。虽然肯尼亚基于机构的艾滋病毒检测服务(HTS)很有效,但急诊科(ED)的服务提供有限,尽管有潜力覆盖到服务不足的人群。
这项准实验性前瞻性研究评估了肯尼亚内罗毕肯雅塔国家医院急诊科的急诊科艾滋病毒强化检测与服务(HEATED)项目的实施情况。HEATED项目利用特定场所的数据进行设计,并通过资源重组、服务整合和艾滋病毒宣传来促进急诊科艾滋病毒检测服务。重点人群包括性工作者、男同性恋者、与男性发生性关系的男性、跨性别者和注射吸毒者。优先人群包括年轻人(18 - 24岁)、人际暴力受害者、有有害酒精使用行为者以及从未接受过艾滋病毒检测的人。数据来自系统层面的记录、登记的受伤患者参与者和医疗服务提供者。在实施前阶段(2023年3月6日至4月16日)和实施后(阶段1,2023年5月1日至6月26日)收集系统和患者层面的数据。此外,在第二个实施后阶段(阶段2,2023年6月27日至8月20日)收集系统层面的数据。评估分析在覆盖范围、有效性、采用情况、实施情况和维持框架领域完成。
通过对HEATED项目的培训和宣传,覆盖了所有151名临床工作人员。系统层面的急诊科艾滋病毒检测服务从实施前的16.7%增加到实施后阶段1和阶段2的23.0%(相对风险 = 1.31,95%置信区间:1.21 - 1.43;p < 0.001),艾滋病毒自检试剂盒的提供相对增加了62.9%。在605名患者参与者中,基于机构的艾滋病毒检测服务从实施前的5.7%增加到实施后阶段1的62.3%(相对风险 = 11.2,95%置信区间:6.9 - 18.1;p < 0.001)。有440名(72.7%)患者参与者被确定为重点人群(5.6%)和/或优先人群(65.3%)。对于登记的重点人群/优先人群,艾滋病毒检测服务从实施前的4.6%增加到实施后阶段1的72.3%(相对风险 = 13.8,95%置信区间:5.5 - 28.7,p < 0.001)。系统和参与者层面的数据表明HEATED项目成功被采用和实施。在实施后16周内,与实施前相比,急诊科艾滋病毒检测服务的提供量持续显著增加。
HEATED项目增加了急诊科艾滋病毒检测服务,并扩大了对重点人群/优先人群的服务提供,这表明更广泛的实施可以改善已经与卫生系统有接触的服务不足人群的艾滋病毒服务。