Department of Emergency Medicine, Kaiser Permanente Medical Center, Oakland, California.
Department of Critical Care Medicine, Kaiser Permanente Medical Center, Oakland, California.
JAMA Netw Open. 2024 Apr 1;7(4):e247373. doi: 10.1001/jamanetworkopen.2024.7373.
Subarachnoid hemorrhage is typically diagnosed by noncontrast head computed tomography (CT); lumbar puncture is recommended if computed tomography is nondiagnostic, although CT cerebral angiography has been promoted as an alternative to lumbar puncture in this diagnostic pathway. The outcomes of this debate in practice have not been studied.
To determine whether CT cerebral angiography use has increased in lieu of lumbar puncture among emergency department (ED) patients with headache, with an increase in unruptured intracranial aneurysm detection.
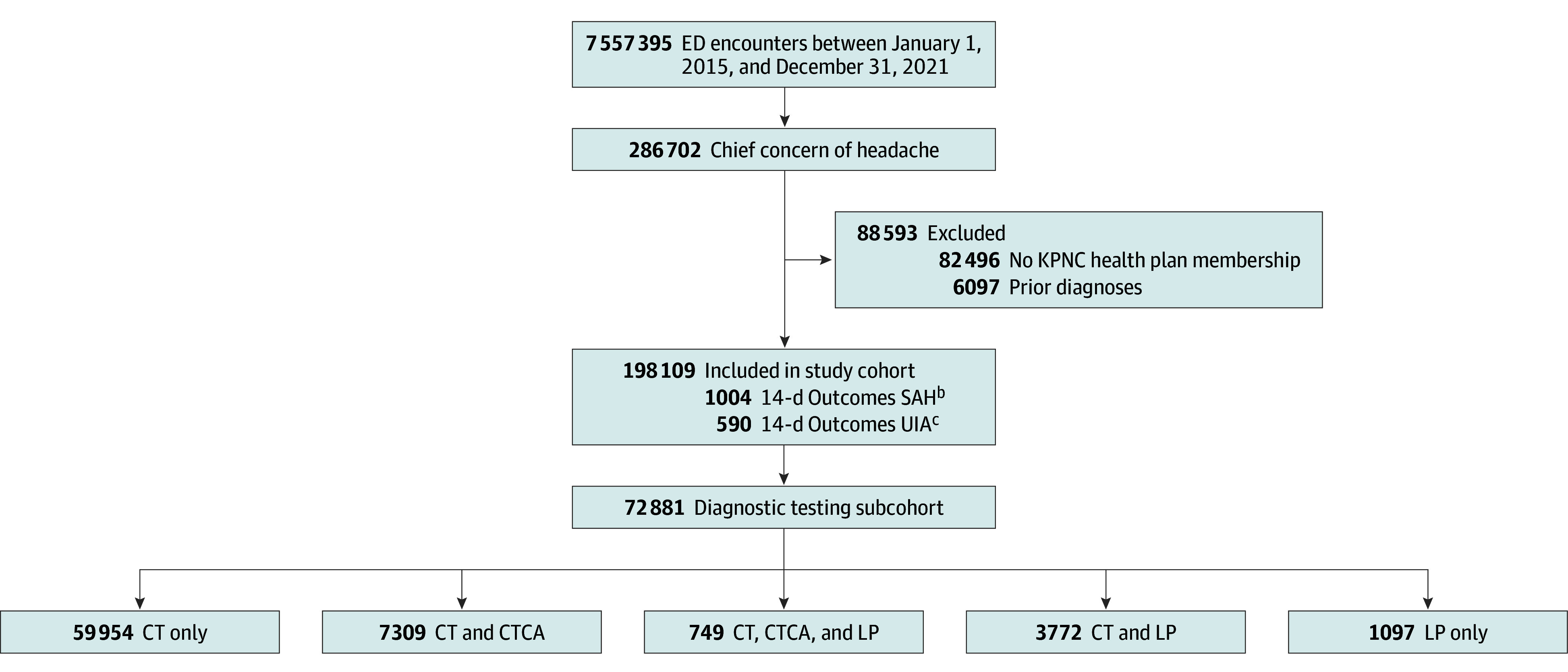
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study took place in 21 community EDs of an integrated health care system in Northern California between 2015 and 2021. Participants were adult (aged >17 years) health plan members with a chief concern of headache. Exclusions were prior diagnoses of subarachnoid hemorrhage, unruptured intracranial aneurysm, cerebral arteriovenous malformation, or cerebrospinal fluid shunt. Data were analyzed from October to November 2023.
CT cerebral angiography and/or lumbar puncture during the ED encounter.
Primary and secondary outcomes were 14-day and 90-day unruptured intracranial aneurysm detection, respectively. Safety outcomes were missed diagnoses of subarachnoid hemorrhage or bacterial meningitis. The annual incidence of unruptured intracranial aneurysm detection was normalized to the incidence of subarachnoid hemorrhage (UIA:SAH ratio). Average annualized percentage changes were quantified using joinpoint regression analysis.
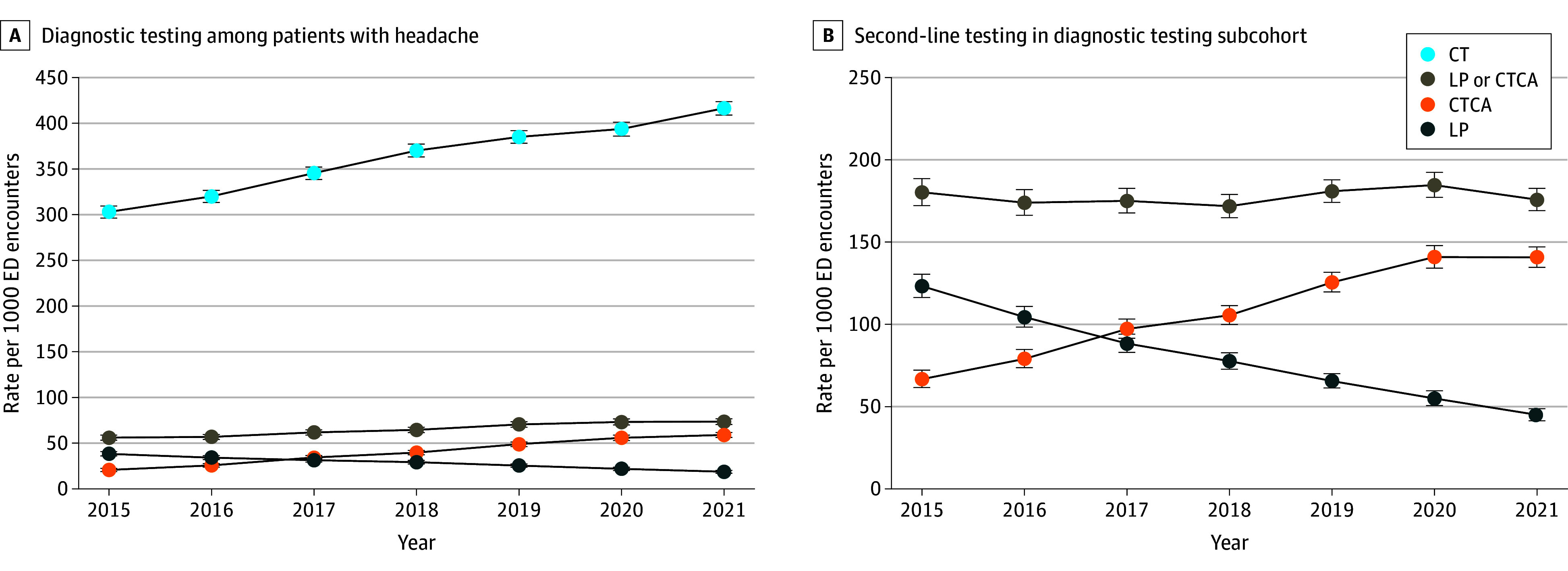
Among 198 109 included ED encounters, the mean (SD) age was 47.5 (18.4) years; 140 001 patients (70.7%) were female; 29 035 (14.7%) were Black or African American, 59 896 (30.2%) were Hispanic or Latino, and 75 602 (38.2%) were White. Per year, CT cerebral angiography use increased (18.8%; 95% CI, 17.7% to 20.3%) and lumbar punctures decreased (-11.1%; 95% CI, -12.0% to -10.4%), with a corresponding increase in the 14-day UIA:SAH ratio (3.5%; 95% CI, 0.9% to 7.4%). Overall, computed tomography cerebral angiography use increased 6-fold relative to lumbar puncture, with a 33% increase in the detection of UIA. Results were similar at 90 days and robust to sensitivity analyses. Subarachnoid hemorrhage (1004 cases) and bacterial meningitis (118 cases) were misdiagnosed in 5% and 18% of cases, respectively, with no annual trends (P = .34; z1003 = .95 and P = .74; z117 = -.34, respectively).
In this cohort study of ED patients with headache, increases in CT cerebral angiography use were associated with fewer lumbar punctures and higher detection of unruptured intracranial aneurysms, with no significant change in missed diagnoses of subarachnoid hemorrhage or bacterial meningitis. While this shift in diagnostic strategy appeared safe in the short-term, the long-term consequences remain unclear.
蛛网膜下腔出血通常通过非对比头部计算机断层扫描 (CT) 进行诊断;如果 CT 检查结果不可诊断,建议进行腰椎穿刺,尽管 CT 脑血管造影术已被推荐作为该诊断途径中腰椎穿刺的替代方法。这一争论在实践中的结果尚未得到研究。
确定在头痛的急诊科 (ED) 患者中,CT 脑血管造影术的使用是否已取代腰椎穿刺,同时增加未破裂颅内动脉瘤的检出率。
设计、地点和参与者:这是一项回顾性队列研究,在北加州一个综合医疗保健系统的 21 个社区急诊科进行,时间为 2015 年至 2021 年。参与者为年龄大于 17 岁的成年 (健康计划) 成员,主要关注头痛。排除标准为先前诊断为蛛网膜下腔出血、未破裂颅内动脉瘤、脑动静脉畸形或脑脊髓液分流。数据于 2023 年 10 月至 11 月进行分析。
ED 就诊期间进行 CT 脑血管造影术和/或腰椎穿刺。
主要和次要结果分别为 14 天和 90 天未破裂颅内动脉瘤的检出率。安全性结果为蛛网膜下腔出血或细菌性脑膜炎的漏诊。未破裂颅内动脉瘤的检出率以蛛网膜下腔出血的发生率为归一化(未破裂颅内动脉瘤:蛛网膜下腔出血比,UIA:SAH 比)。使用 Joinpoint 回归分析量化平均年化百分比变化。
在 198109 例纳入的 ED 就诊中,平均(SD)年龄为 47.5(18.4)岁;140001 例患者(70.7%)为女性;29035 例(14.7%)为黑人或非裔美国人,59896 例(30.2%)为西班牙裔或拉丁裔,75602 例(38.2%)为白人。每年,CT 脑血管造影术的使用增加(18.8%;95%CI,17.7%至 20.3%),腰椎穿刺减少(-11.1%;95%CI,-12.0%至-10.4%),相应的 14 天 UIA:SAH 比增加(3.5%;95%CI,0.9%至 7.4%)。总体而言,与腰椎穿刺相比,计算机断层血管造影术的使用增加了 6 倍,未破裂颅内动脉瘤的检出率增加了 33%。90 天的结果相似,且对敏感性分析具有稳健性。蛛网膜下腔出血(1004 例)和细菌性脑膜炎(118 例)的误诊率分别为 5%和 18%,无年度趋势(P = .34;z1003 = .95 和 P = .74;z117 = -.34,分别)。
在这项头痛急诊科患者的队列研究中,CT 脑血管造影术使用率的增加与腰椎穿刺次数减少和未破裂颅内动脉瘤检出率增加相关,蛛网膜下腔出血或细菌性脑膜炎漏诊率无显著变化。虽然这一诊断策略的转变在短期内似乎是安全的,但长期后果仍不清楚。