Gill Harman Singh, Marcolini Evie Grace, Barber Douglas, Wira Charles R
Department of Emergency Medicine, Yale New Haven Hospital, New Haven, CT.
Departments of Emergency Medicine and Neurology, Divisions of Neurocritical Care and Emergency Neurology and Surgical Critical Care, Yale University School of Medicine, Yale New Haven Hospital, New Haven, CT.
Yale J Biol Med. 2018 Mar 28;91(1):3-11. eCollection 2018 Mar.
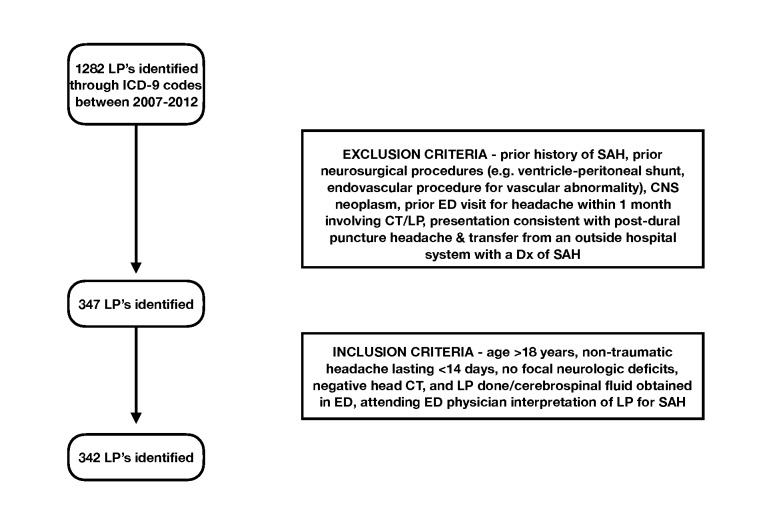
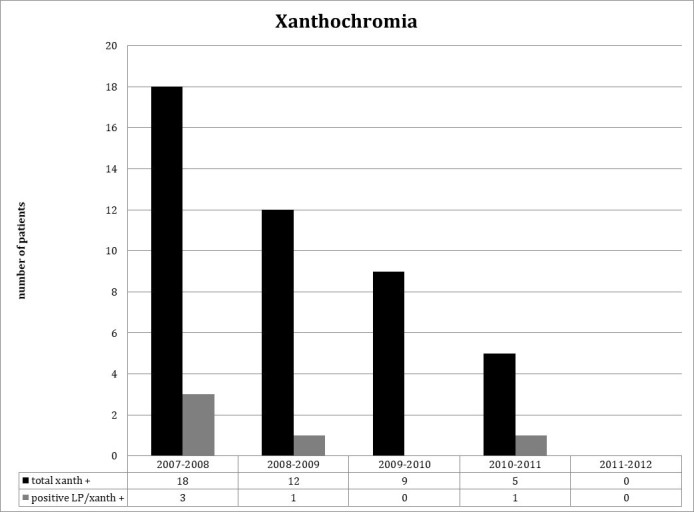
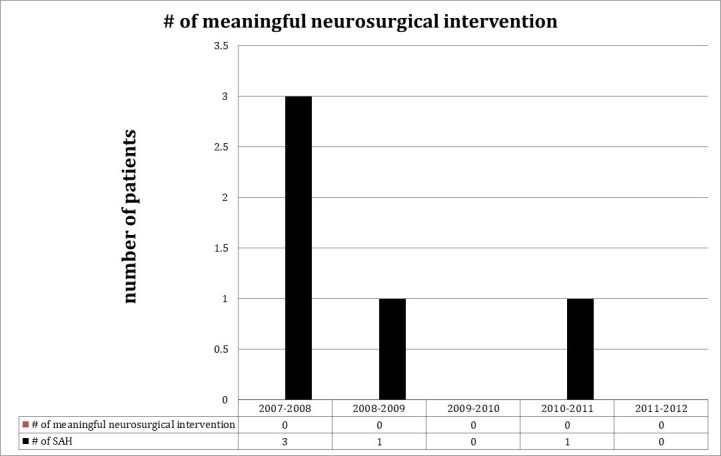
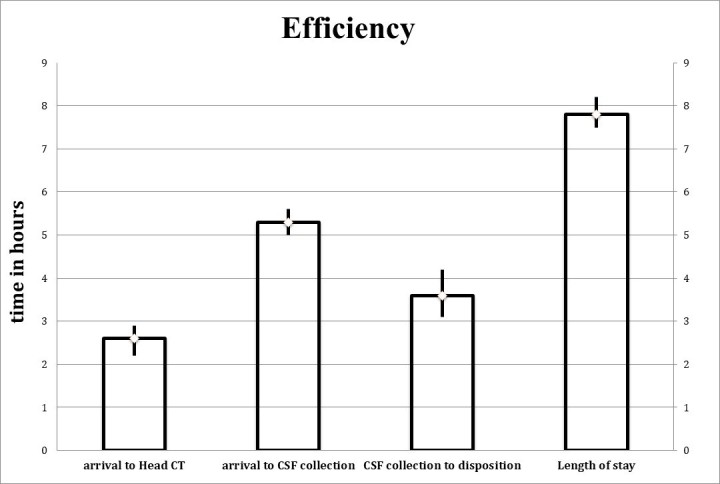
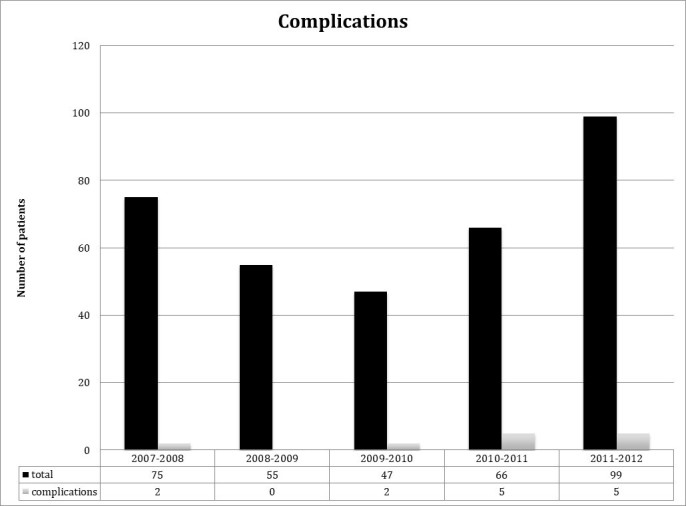
American College of Emergency Physicians (ACEP) [1] recommends that patients presenting with acute non-traumatic headache concerning for subarachnoid hemorrhage (SAH) undergo lumbar puncture (LP) when non-contrast head computed tomography (CT) is negative. The diagnostic yield of this approach is unknown. Evaluate the diagnostic yield, lengths of stay and complication rates of LPs in patients undergoing Emergency Department (ED) evaluation for aneurysmal SAH. Multi-center, retrospective, hypothesis-blinded, explicit chart review of patients undergoing ED-based lumbar puncture between 2007 and 2012. Charts of neurologically intact patients presenting with headache that had a negative head CT and underwent LP primarily to rule out SAH were reviewed. Trained data abstractors blinded to study hypothesis used standardized data forms with predefined terms for chart abstraction. We re-abstracted and assessed inter-rater agreement for 20 percent of charts with a 100 percent inter-rater agreement. Data were descriptive, using 95 percent confidence intervals. 1,282 LPs were performed, and 342 patients met inclusion criteria but only 1 percent were deemed positive for SAH in the chart. No aneurysm or vascular malformation was identified in those with positive LPs for SAH. Complications were in 4 percent and xanthochromia was found in 13 percent. Total length of stay was 7.8 hours (0.95 CI; 7.5 - 8.2). No patient discharged from the ED after a negative workup for SAH was re-admitted for SAH or underwent a neurosurgical procedure during a three-month follow-up period. LP in our cohort of neurologically intact CT-negative ED headache patients did not identify any cases of aneurysmal SAH but was associated with serious complications, a significant false positive rate, and extended ED length of stay.
美国急诊医师学会(ACEP)[1]建议,对于因蛛网膜下腔出血(SAH)而出现急性非创伤性头痛的患者,在非增强头部计算机断层扫描(CT)结果为阴性时应进行腰椎穿刺(LP)。这种方法的诊断率尚不清楚。评估在急诊科(ED)接受动脉瘤性SAH评估的患者中LP的诊断率、住院时间和并发症发生率。对2007年至2012年间在急诊科接受基于腰椎穿刺的患者进行多中心、回顾性、假设盲法、明确的病历审查。审查了神经系统完好、头痛且头部CT阴性、主要为排除SAH而进行LP的患者的病历。对研究假设不知情的经过培训的数据提取人员使用具有预定义术语的标准化数据表格进行病历提取。我们对20%的病历进行了重新提取并评估了评分者间的一致性,评分者间一致性为100%。数据采用描述性分析,使用95%置信区间。共进行了1282次腰椎穿刺,342例患者符合纳入标准,但病历中仅1%被判定为SAH阳性。SAH腰椎穿刺阳性的患者中未发现动脉瘤或血管畸形。并发症发生率为4%,发现黄变的比例为13%。总住院时间为7.8小时(0.95置信区间;7.5 - 8.2)。在SAH检查结果为阴性后从急诊科出院的患者,在三个月的随访期内没有因SAH再次入院或接受神经外科手术。在我们这组神经系统完好、CT阴性的急诊科头痛患者中,腰椎穿刺未发现任何动脉瘤性SAH病例,但与严重并发症、显著的假阳性率和延长的急诊科住院时间相关。