Department of Surgery, Radboud University Medical Center, Nijmegen, the Netherlands.
IQ Healthcare, Radboud University Medical Center, Nijmegen, the Netherlands.
JAMA Netw Open. 2024 Apr 1;7(4):e246556. doi: 10.1001/jamanetworkopen.2024.6556.
Suboptimal surgical performance is hypothesized to be associated with less favorable patient outcomes in minimally invasive esophagectomy (MIE). Establishing this association may lead to programs that promote better surgical performance of MIE and improve patient outcomes.
To investigate associations between surgical performance and postoperative outcomes after MIE.
DESIGN, SETTING, AND PARTICIPANTS: In this nationwide cohort study of 15 Dutch hospitals that perform more than 20 MIEs per year, 7 masked expert MIE surgeons assessed surgical performance using videos and a previously developed and validated competency assessment tool (CAT). Each hospital submitted 2 representative videos of MIEs performed between November 4, 2021, and September 13, 2022. Patients registered in the Dutch Upper Gastrointestinal Cancer Audit between January 1, 2020, and December 31, 2021, were included to examine patient outcomes.
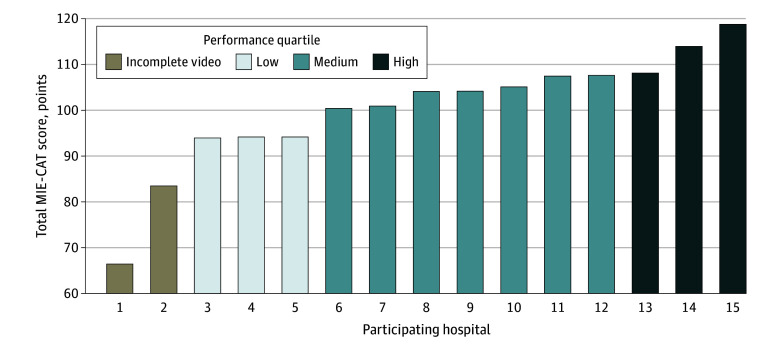
Hospitals were divided into quartiles based on their MIE-CAT performance score. Outcomes were compared between highest (top 25%) and lowest (bottom 25%) performing quartiles. Transthoracic MIE with gastric tube reconstruction.
The primary outcome was severe postoperative complications (Clavien-Dindo ≥3) within 30 days after surgery. Multilevel logistic regression, with clustering of patients within hospitals, was used to analyze associations between performance and outcomes.
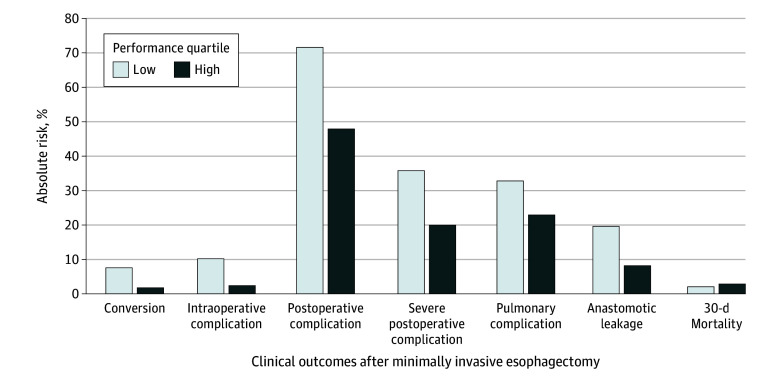
In total, 30 videos and 970 patients (mean [SD] age, 66.6 [9.1] years; 719 men [74.1%]) were included. The mean (SD) MIE-CAT score was 113.6 (5.5) in the highest performance quartile vs 94.1 (5.9) in the lowest. Severe postoperative complications occurred in 18.7% (41 of 219) of patients in the highest performance quartile vs 39.2% (40 of 102) in the lowest (risk ratio [RR], 0.50; 95% CI, 0.24-0.99). The highest vs the lowest performance quartile showed lower rates of conversions (1.8% vs 8.9%; RR, 0.21; 95% CI, 0.21-0.21), intraoperative complications (2.7% vs 7.8%; RR, 0.21; 95% CI, 0.04-0.94), and overall postoperative complications (46.1% vs 65.7%; RR, 0.54; 95% CI, 0.24-0.96). The R0 resection rate (96.8% vs 94.2%; RR, 1.03; 95% CI, 0.97-1.05) and lymph node yield (mean [SD], 38.9 [14.7] vs 26.2 [9.0]; RR, 3.20; 95% CI, 0.27-3.21) increased with oncologic-specific performance (eg, hiatus dissection, lymph node dissection). In addition, a high anastomotic phase score was associated with a lower anastomotic leakage rate (4.6% vs 17.7%; RR, 0.14; 95% CI, 0.06-0.31).
These findings suggest that better surgical performance is associated with fewer perioperative complications for patients with esophageal cancer on a national level. If surgical performance of MIE can be improved with MIE-CAT implementation, substantially better patient outcomes may be achievable.
微创食管切除术(MIE)中较差的手术表现被假设与患者术后结果较差有关。确定这种关联可能会导致实施促进 MIE 手术表现更好和改善患者结果的方案。
调查 MIE 后手术表现与术后结果之间的关联。
设计、设置和参与者:在这项对每年进行超过 20 例 MIE 的 15 家荷兰医院的全国性队列研究中,7 名盲法 MIE 专家使用视频和先前开发和验证的能力评估工具(CAT)评估手术表现。每家医院提交了 2 例在 2021 年 11 月 4 日至 2022 年 9 月 13 日期间进行的 MIE 的代表性视频。包括 2020 年 1 月 1 日至 2021 年 12 月 31 日期间在荷兰上消化道癌症审计中注册的患者,以检查患者的结果。
根据 MIE-CAT 表现评分将医院分为四分位组。比较最高(前 25%)和最低(后 25%)四分位组之间的结果。经胸 MIE 加胃管重建。
主要结果是手术后 30 天内发生严重术后并发症(Clavien-Dindo ≥3)。使用多水平逻辑回归,对医院内的患者进行聚类分析,分析表现与结果之间的关联。
共纳入 30 个视频和 970 例患者(平均[标准差]年龄,66.6[9.1]岁;719 名男性[74.1%])。最高表现四分位组的 MIE-CAT 评分平均(标准差)为 113.6(5.5),而最低表现四分位组为 94.1(5.9)。最高表现四分位组有 18.7%(41/219)的患者发生严重术后并发症,而最低表现四分位组有 39.2%(40/102)(风险比[RR],0.50;95%CI,0.24-0.99)。与最低四分位组相比,最高四分位组的转换率(1.8% vs 8.9%;RR,0.21;95%CI,0.21-0.21)、术中并发症(2.7% vs 7.8%;RR,0.21;95%CI,0.04-0.94)和总术后并发症(46.1% vs 65.7%;RR,0.54;95%CI,0.24-0.96)较低。R0 切除率(96.8% vs 94.2%;RR,1.03;95%CI,0.97-1.05)和淋巴结产量(平均值[标准差],38.9[14.7] vs 26.2[9.0];RR,3.20;95%CI,0.27-3.21)随着肿瘤特异性表现(例如,裂孔解剖、淋巴结清扫)的增加而增加。此外,吻合口阶段评分较高与吻合口漏发生率较低相关(4.6% vs 17.7%;RR,0.14;95%CI,0.06-0.31)。
这些发现表明,在全国范围内,更好的手术表现与食管癌患者围手术期并发症较少相关。如果 MIE-CAT 的实施可以提高 MIE 的手术表现,可能会实现更好的患者结果。