New York University Grossman School of Medicine, New York, NY.
Division of Vascular and Endovascular Surgery, Department of Surgery, New York University Langone Health, New York, NY.
J Vasc Surg Venous Lymphat Disord. 2024 Sep;12(5):101898. doi: 10.1016/j.jvsv.2024.101898. Epub 2024 Apr 25.
Endovenous ablation is the standard of care for patients with symptomatic superficial venous insufficiency. For patients with a history of deep vein thrombosis (DVT), concern exists for an increased risk of postprocedural complications, particularly venous thromboembolism. The objective of this study was to evaluate the safety and efficacy of endovenous thermal ablation in patients with a history of DVT.
The national Vascular Quality Initiative Varicose Vein Registry was queried for superficial venous procedures performed from January 2014 to July 2021. Limbs treated with radiofrequency or laser ablation were compared between patients with and without a DVT history. The primary safety end point was incident DVT or endothermal heat-induced thrombosis (EHIT) II-IV in the treated limb at <3 months of follow-up. The secondary safety end points included any proximal thrombus extension (ie, EHIT I-IV), major bleeding, hematoma, pulmonary embolism, and death due to the procedure. The primary efficacy end point was technical failure (ie, recanalization at <1 week of follow-up). Secondary efficacy end points included the risk of recanalization over time and the postprocedural change in quality-of-life measures. Outcomes stratified by preoperative use of anticoagulation (AC) were also compared among those with prior DVT.
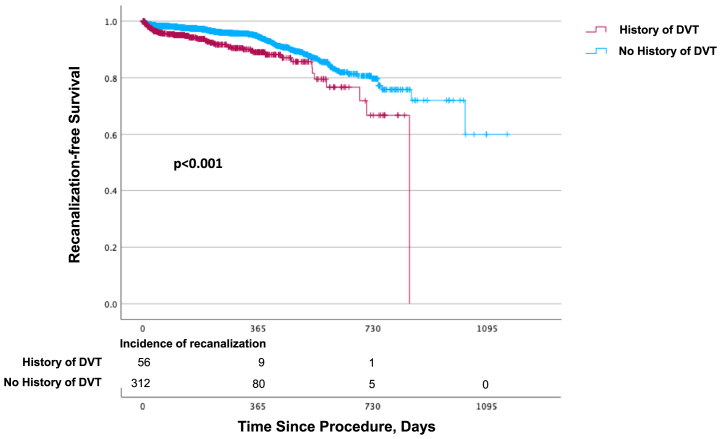
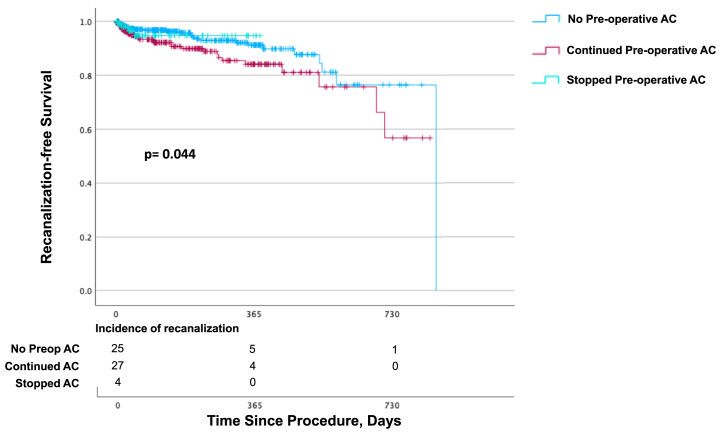
Among 33,892 endovenous thermal ablations performed on 23,572 individual patients aged 13 to 90 years, 1698 patients (7.2%) had a history of DVT. Patients with prior DVT were older (P < .001), had a higher body mass index (P < .001), were more likely to be male at birth (P < .001) and Black/African American (P < .001), and had greater CEAP classifications (P < .001). A history of DVT conferred a higher risk of new DVT (1.4% vs 0.8%; P = .03), proximal thrombus extension (2.3% vs 1.6%; P = .045), and bleeding (0.2% vs 0.04%; P = .03). EHIT II-IV, pulmonary embolism, and hematoma risk did not differ by DVT history (P = NS). No deaths from treatment occurred in either group. Continuing preoperative AC in patients with prior DVT did not change the risk of any complications after endovenous ablation (P = NS) but did confer an increased hematoma risk among all endovenous thermal ablations and surgeries (P = .001). Technical failure was similar between groups (2.0% vs 1.2%; P = .07), although a history of DVT conferred an increased recanalization risk over time (hazard ratio, 1.90; 95% confidence interval, 1.46, 2.46; P < .001). The groups had comparable improvements in postprocedural venous clinical severity scores and Heaviness, Aching, Swelling, Throbbing, and Itching scores (P = NS).
Endovenous thermal ablation for patients with a history of DVT was effective. However, appropriate patient counseling regarding a heightened DVT risk, albeit still low, is critical. The decision to continue or withhold AC preoperatively should be tailored on a case-by-case basis.
静脉内消融是有症状的浅静脉功能不全患者的标准治疗方法。对于有深静脉血栓形成(DVT)病史的患者,存在术后并发症风险增加的担忧,尤其是静脉血栓栓塞症。本研究的目的是评估静脉内热消融治疗有 DVT 病史患者的安全性和疗效。
国家血管质量倡议静脉曲张登记处检索了 2014 年 1 月至 2021 年 7 月期间进行的浅静脉手术。比较了射频或激光消融治疗的肢体在有和无 DVT 病史的患者之间。主要安全性终点是治疗肢体在<3 个月随访时发生的新发 DVT 或热诱导血栓形成(EHIT)II-IV。次要安全性终点包括任何近端血栓延伸(即 EHIT I-IV)、大出血、血肿、肺栓塞和因手术导致的死亡。主要疗效终点是技术失败(即<1 周随访时再通)。次要疗效终点包括随时间推移再通的风险和术后生活质量测量的变化。还比较了术前使用抗凝剂(AC)的分层结果。
在 23572 名年龄为 13 至 90 岁的个体中进行了 33892 次静脉内热消融治疗,其中 1698 名患者(7.2%)有 DVT 病史。有 DVT 病史的患者年龄较大(P<0.001)、体重指数较高(P<0.001)、更有可能在出生时为男性(P<0.001)和黑/非裔美国人(P<0.001),且 CEAP 分类更高(P<0.001)。DVT 病史使新发 DVT 的风险更高(1.4% vs 0.8%;P=0.03)、近端血栓延伸的风险更高(2.3% vs 1.6%;P=0.045)和出血风险更高(0.2% vs 0.04%;P=0.03)。EHIT II-IV、肺栓塞和血肿风险与 DVT 病史无关(P=NS)。两组均无治疗相关死亡。在有 DVT 病史的患者中继续术前 AC 并不会改变静脉内消融后的任何并发症风险(P=NS),但会增加所有静脉内热消融和手术的血肿风险(P=0.001)。两组之间的技术失败率相似(2.0% vs 1.2%;P=0.07),但 DVT 病史会增加随时间再通的风险(危险比,1.90;95%置信区间,1.46,2.46;P<0.001)。两组术后静脉临床严重程度评分和沉重感、疼痛、肿胀、悸动和瘙痒评分均有改善(P=NS)。
对于有 DVT 病史的患者,静脉内热消融是有效的。然而,需要对患者进行适当的咨询,告知他们存在较高的 DVT 风险,尽管这种风险仍然较低。是否继续或停止术前 AC 应根据具体情况决定。