Department of Surgery, Division of Surgical Sciences, Columbia University Irving Medical Center, New York, New York.
Caris Life Sciences, Phoenix, Arizona.
Cancer Res Commun. 2024 Jun 3;4(6):1399-1409. doi: 10.1158/2767-9764.CRC-23-0496.
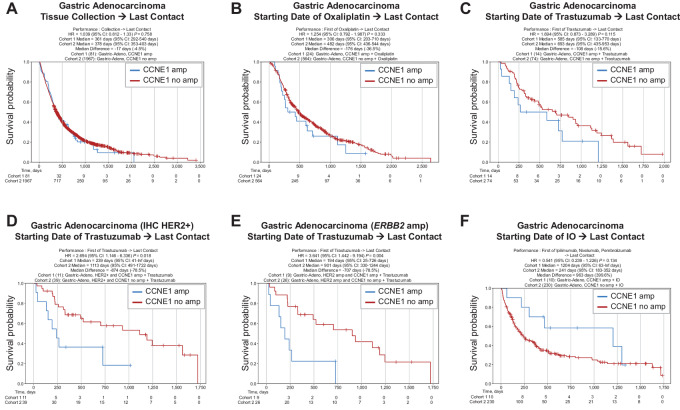
Cyclin E overexpression as a result of CCNE1 amplification is a critical driver of genomic instability in gastric cancer, but its clinical implication is largely unknown. Thus, we integrated genomic, transcriptomic, and immune profiling analysis of 7,083 esophagogastric tumors and investigated the impact of CCNE1 amplification on molecular features and treatment outcomes. We identified CCNE1 amplification in 6.2% of esophageal adenocarcinoma samples, 7.0% of esophagogastric junction carcinoma, 4.2% of gastric adenocarcinoma samples, and 0.8% of esophageal squamous cell carcinoma. Metastatic sites such as lymph node and liver showed an increased frequency of CCNE1 amplification relative to primary tumors. Consistent with a chromosomal instability phenotype, CCNE1 amplification was associated with decreased CDH1 mutation and increased TP53 mutation and ERBB2 amplification. We observed no differences in immune biomarkers such as PD-L1 expression and tumor mutational burden comparing CCNE1-amplified and nonamplified tumors, although CCNE1 amplification was associated with changes in immune populations such as decreased B cells and increased M1 macrophages from transcriptional analysis. Real-world survival analysis demonstrated that patients with CCNE1-amplified gastric cancer had worse survival after trastuzumab for HER2-positive tumors, but better survival after immunotherapy. These data suggest that CCNE1-amplified gastric cancer has a distinct molecular and immune profile with important therapeutic implications, and therefore further investigation of CCNE1 amplification as a predictive biomarker is warranted.
Advanced gastric cancer has a relatively dismal outcome with a 5-year overall survival of less than 10%. Furthermore, while comprehensive molecular analyses have established molecular subtypes within gastric cancers, biomarkers of clinical relevance in this cancer type are lacking. Overall, this study demonstrates that CCNE1 amplification is associated with a distinct molecular profile in gastric cancer and may impact response to therapy, including targeted therapy and/or immunotherapy.
CCNE1 扩增导致的细胞周期蛋白 E 过表达是胃癌基因组不稳定的关键驱动因素,但它的临床意义在很大程度上尚不清楚。因此,我们整合了 7083 例食管胃肿瘤的基因组、转录组和免疫分析,研究了 CCNE1 扩增对分子特征和治疗结果的影响。我们在 6.2%的食管腺癌样本、7.0%的食管胃交界癌、4.2%的胃腺癌样本和 0.8%的食管鳞状细胞癌中发现了 CCNE1 扩增。与原发肿瘤相比,淋巴结和肝脏等转移部位 CCNE1 扩增的频率增加。与染色体不稳定表型一致,CCNE1 扩增与 CDH1 突变减少、TP53 突变和 ERBB2 扩增增加相关。与 CCNE1 扩增和非扩增肿瘤相比,我们没有观察到免疫生物标志物如 PD-L1 表达和肿瘤突变负担的差异,尽管 CCNE1 扩增与免疫群体的变化相关,如转录分析中 B 细胞减少和 M1 巨噬细胞增加。真实世界的生存分析表明,曲妥珠单抗治疗 HER2 阳性肿瘤时,CCNE1 扩增的胃癌患者的生存较差,但免疫治疗后生存较好。这些数据表明,CCNE1 扩增的胃癌具有独特的分子和免疫特征,具有重要的治疗意义,因此需要进一步研究 CCNE1 扩增作为预测生物标志物。
晚期胃癌的总体 5 年生存率低于 10%,预后较差。此外,尽管全面的分子分析已经确定了胃癌的分子亚型,但这种癌症类型缺乏临床相关的生物标志物。总的来说,这项研究表明,CCNE1 扩增与胃癌的独特分子谱相关,可能影响治疗反应,包括靶向治疗和/或免疫治疗。