Faculty of Medicine, University of Iceland, Reykjavik, Iceland.
Department of Urology and Surgery in Landspitali University Hospital, Reykjavik, Iceland.
BMC Urol. 2024 May 13;24(1):105. doi: 10.1186/s12894-024-01494-9.
Papillary renal cell carcinoma (pRCC) is the second most common histology of renal cell carcinoma (RCC), accounting for 10-15% of cases. Traditionally, pRCC is divided into type 1 and type 2, although this division is currently debated as a prognostic factor of survival. Our aim was to investigate the epidemiology and survival of the pRCC subtypes in a whole nation cohort of patients during a 50-year period.
A Population based retrospective study including consecutive cases of RCC in Iceland from 1971-2020. Comparisons were made between histological classifications of RCC, with emphasis on pRCC subtypes (type 1 vs. 2) for outcome estimation. Changes in RCC incidence were analyzed in 5-year intervals after age standardization. The Kaplan-Meier method and Cox regression were used for outcome analysis.
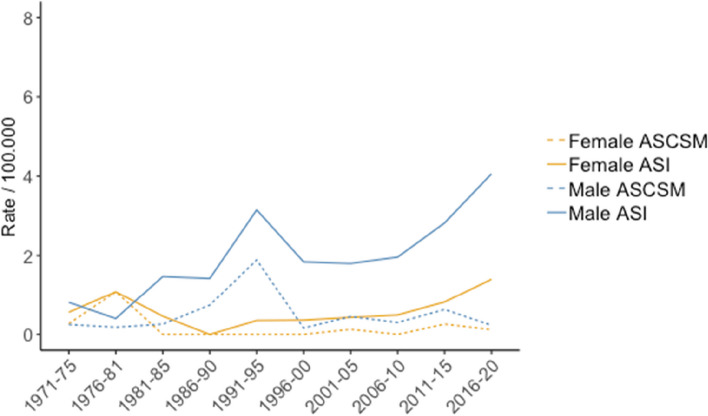
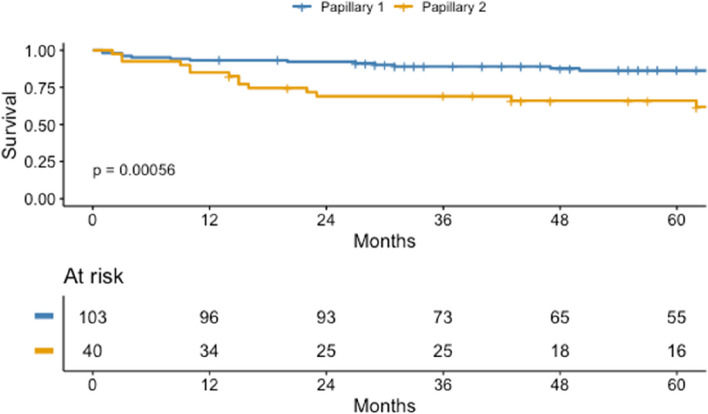
A total of 1.725 cases were identified, with 74.4%, 2.1% and 9.2% having clear cell (ccRCC), chromophobe (chRCC), and pRCC, respectively. The age standardized incidence (ASI) of pRCC was 1.97/100.000 for males and 0.5/100.000 for females, and the proportion of pRCC increased from 3.7% to 11.5% between the first and last intervals of the study (p < 0.001). Age standardized cancer specific mortality (ASCSM) of pRCC was 0.6/100.000 and 0.19/100.000 for males and females, respectively. The annual average increase in ASI was 3.6% for type 1 pRCC, but the ASI for type 2 pRCC and ASCSM for both subtypes did not change significantly. Male to female ratio was 4.4 for type 1 pRCC and 2.3 for type 2. The average tumor size for type 1 and 2 was 58.8 and 73.7 mm, respectively. Metastasis at diagnosis was found in 8.7% in the type 1 pRCC, compared to 30.0% of patients with type 2 pRCC (p < 0.001). Estimated 5-year cancer-specific survival (CSS) were 94.4%, 80.7%, and 69.3% for chRCC, pRCC and ccRCC, respectively (p < 0.001). For the pRCC subtypes, type 1 was associated with better 5-year CSS than type 2 (86.3% vs. 66.0%, p < 0.001), although this difference was not significant after adjusting for cancer stage and grading.
pRCC histology was slightly less common in Iceland than in other countries. Males are more than three times more likely to be diagnosed with pRCC, compared to other RCC histologies. The subtype of pRCC was not found to be an independent risk factor for worse survival, and as suggested by the most recent WHO Classification of Urinary Tumors, grade and TNM-stage seem to be the most important factors for estimation of survival for pRCC patients.
乳头状肾细胞癌(pRCC)是肾细胞癌(RCC)的第二大常见组织学类型,占病例的 10-15%。传统上,pRCC 分为 1 型和 2 型,尽管目前这一分型作为生存的预后因素存在争议。我们的目的是在 50 年的时间里,在整个国家的患者队列中研究 pRCC 亚型的流行病学和生存情况。
这是一项基于人群的回顾性研究,纳入了 1971 年至 2020 年冰岛连续的 RCC 病例。对 RCC 的组织学分类进行了比较,重点是 pRCC 亚型(1 型与 2 型)的预后评估。对年龄标准化后每 5 年的 RCC 发病率变化进行了分析。使用 Kaplan-Meier 方法和 Cox 回归进行生存分析。
共确定了 1725 例病例,其中透明细胞(ccRCC)、嫌色细胞(chRCC)和 pRCC 分别占 74.4%、2.1%和 9.2%。男性 pRCC 的年龄标准化发病率(ASI)为 1.97/100,000,女性为 0.5/100,000,研究期间第一和最后间隔 pRCC 的比例从 3.7%增加到 11.5%(p<0.001)。pRCC 的年龄标准化癌症特异性死亡率(ASCSM)分别为男性 0.6/100,000 和女性 0.19/100,000。1 型 pRCC 的 ASI 平均每年增加 3.6%,但 2 型 pRCC 的 ASI 和两种亚型的 ASCSM 均无显著变化。1 型 pRCC 的男女比例为 4.4,2 型为 2.3。1 型和 2 型的平均肿瘤大小分别为 58.8 和 73.7 毫米。1 型 pRCC 诊断时发现转移的比例为 8.7%,而 2 型 pRCC 患者为 30.0%(p<0.001)。chRCC、pRCC 和 ccRCC 的估计 5 年癌症特异性生存率(CSS)分别为 94.4%、80.7%和 69.3%(p<0.001)。对于 pRCC 亚型,1 型与 2 型相比,5 年 CSS 更好(86.3%对 66.0%,p<0.001),尽管在调整癌症分期和分级后,这种差异无统计学意义。
pRCC 组织学在冰岛的发病率略低于其他国家。与其他 RCC 组织学类型相比,男性患 pRCC 的可能性是其三倍以上。pRCC 亚型并不是生存的独立危险因素,正如最近的世界卫生组织泌尿系统肿瘤分类所建议的,分级和 TNM 分期似乎是估计 pRCC 患者生存的最重要因素。