Holm Anna, Karlsson Veronika, Nikolajsen Lone, Dreyer Pia
Department of Anesthesiology and Intensive care, Aarhus University Hospital, Palle Juul-Jensens Boulevard 99, 8200 Aarhus N, Denmark.
Department of Health Sciences, University West, Gustava Melins gata 2, S-46132, Trollhättan, Sweden.
Int J Nurs Stud Adv. 2021 Mar 18;3:100025. doi: 10.1016/j.ijnsa.2021.100025. eCollection 2021 Nov.
Nurse-patient communication in intensive care units is challenged by the fact that patients are voiceless due to intubation and mechanical ventilation. Difficult communication affects nurses negatively, and it requires knowledge and expertise to facilitate communication in this complex and technologically tense setting. Augmentative and alternative communication has been suggested as a way of optimising communication; several approaches can be combined in a multi-component intervention. Also, a communication algorithm has been proposed as a way of providing structure in patient communication. To enhance transparency and avoid poorly reported interventions, this paper describes the process, rationale and reflections behind developing a communication intervention called the ICU-COM.
To present the development process of a communication intervention prototype that aims to support and strengthen nurses' communication with mechanically ventilated patients in an intensive care unit.
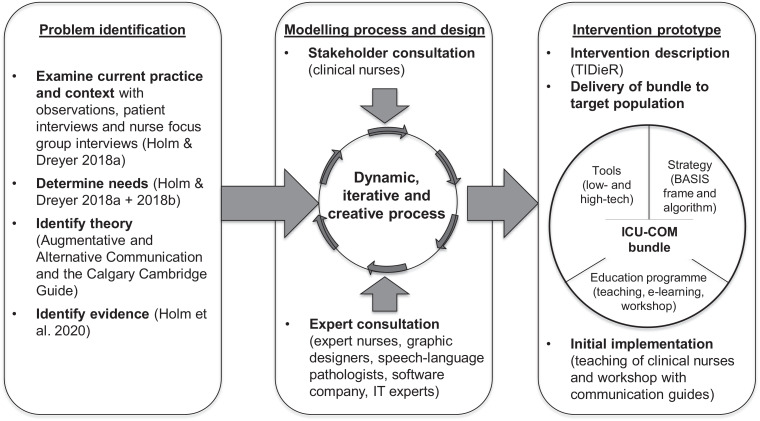
The Medical Research Council's framework for developing complex interventions in health was applied. The approach was target-population centred.
The intervention was developed and tailored to four intensive care unit departments at Aarhus University Hospital in Denmark.
Intensive care nurses and various experts, namely, speech-language pathologists, graphic designers, a software company, the local Centre for E-learning and nurse specialists were involved in its development.
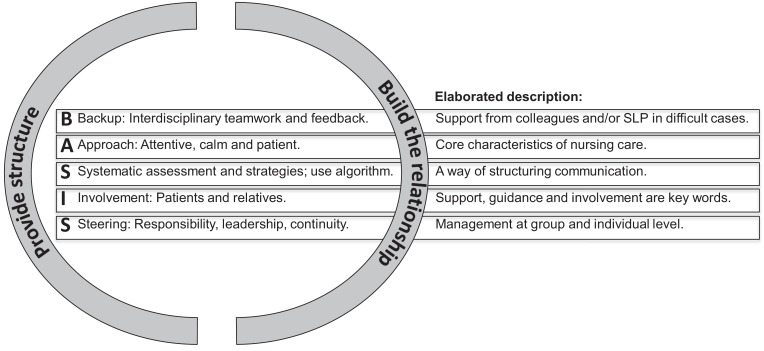
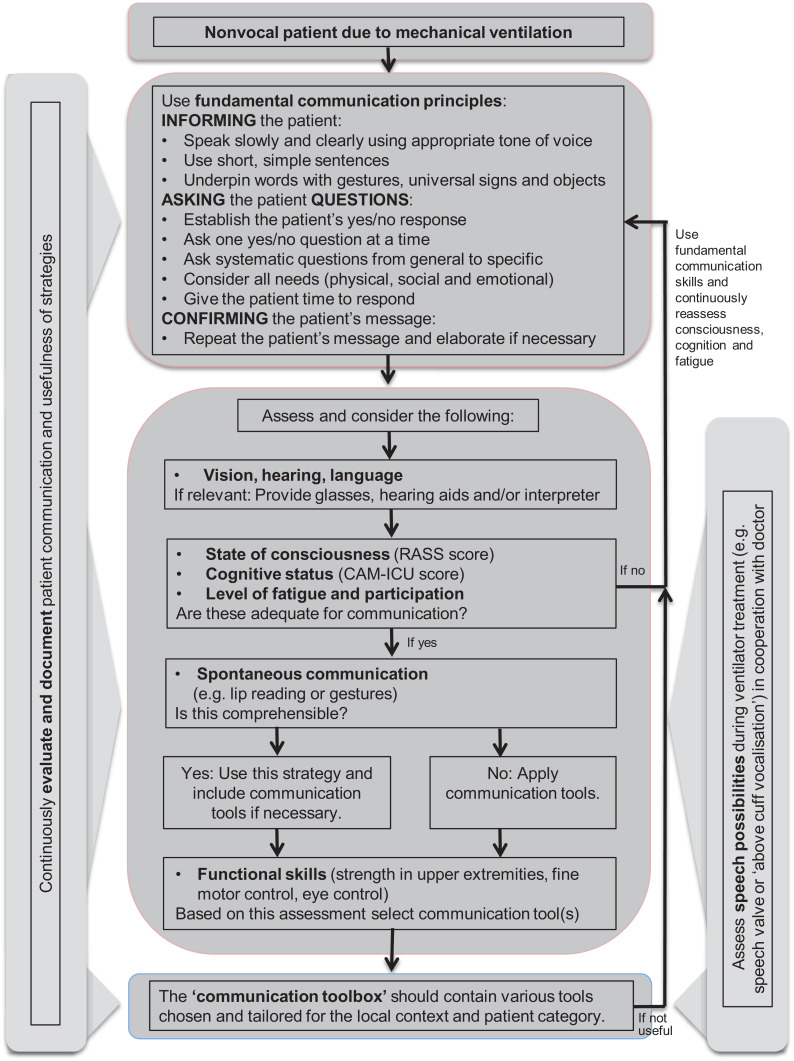
An intervention consisting of: 1) a multi-component communication bundle, 2) delivery of the bundle via a teaching session and 3) initial implementation via nurse communication guides was developed. The communication bundle contained: 1) a communication strategy with a BASIS framework and algorithm, 2) a nurse education programme and 3) low-tech and high-tech communication tools.
A systematic approach was applied in the development process. However, the acceptability and feasibility of the intervention is at present unknown.
重症监护病房中护患沟通面临挑战,因为患者因插管和机械通气而无法发声。沟通困难对护士产生负面影响,在这种复杂且技术氛围紧张的环境中促进沟通需要知识和专业技能。有人建议使用辅助和替代沟通方式来优化沟通;可以将几种方法组合在一个多组件干预措施中。此外,还提出了一种沟通算法,作为在患者沟通中提供结构的一种方式。为提高透明度并避免干预措施报告不佳,本文描述了一种名为ICU-COM的沟通干预措施开发背后的过程、基本原理和思考。
介绍一种沟通干预原型的开发过程,该原型旨在支持和加强重症监护病房中护士与机械通气患者的沟通。
应用了医学研究理事会制定健康领域复杂干预措施的框架。该方法以目标人群为中心。
该干预措施是针对丹麦奥胡斯大学医院的四个重症监护病房部门开发和量身定制的。
重症监护护士和各类专家,即言语治疗师、平面设计师、一家软件公司、当地电子学习中心和护士专家参与了其开发。
开发了一种干预措施,包括:1)一个多组件沟通包,2)通过教学课程提供该包,3)通过护士沟通指南进行初步实施。沟通包包含:1)一个带有BASIS框架和算法的沟通策略,2)一个护士教育计划,3)低技术和高技术沟通工具。
在开发过程中采用了系统方法。然而,目前尚不清楚该干预措施的可接受性和可行性。