Hasan Shaakir, Verma Vivek, Abel Stephen, Wegner Rodney E, Choi J Isabelle, Press Robert H, Chhabra Arpit, Simone Charles B
Department of Radiation Oncology, Allegheny Health Network, Pittsburgh, PA, USA.
New York Proton Center, New York, NY, USA.
Int J Part Ther. 2024 Apr 22;11:100005. doi: 10.1016/j.ijpt.2023.10.001. eCollection 2024 Mar.
To report demographic and clinical characteristics of patients who were more likely to receive proton beam therapy (PBT) than photon therapy from facilities with access to proton centers.
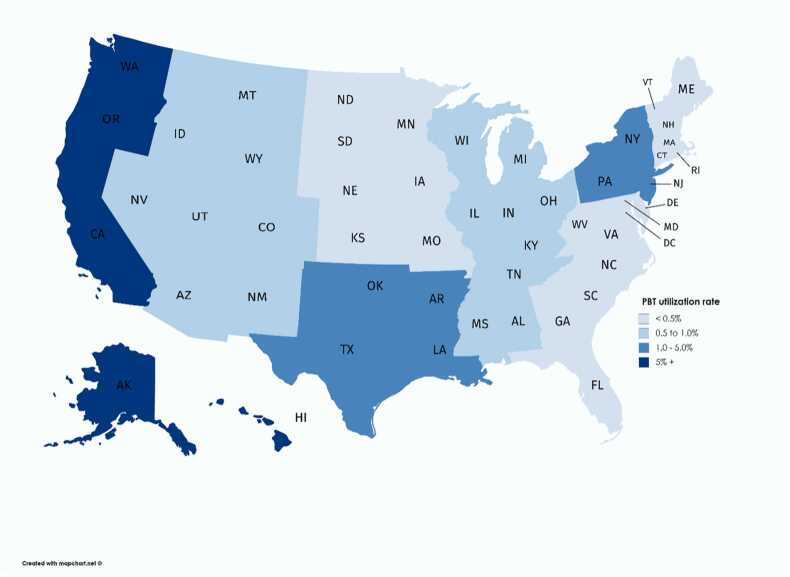
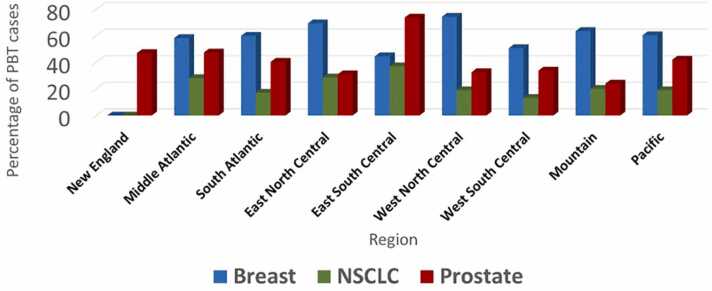
We utilized the national cancer database to identify the facilities with access to PBT between 2004 and 2015 and compared the relative usage of photons and PBT for demographic and clinical scenarios in breast, prostate, and nonsmall cell cancer.
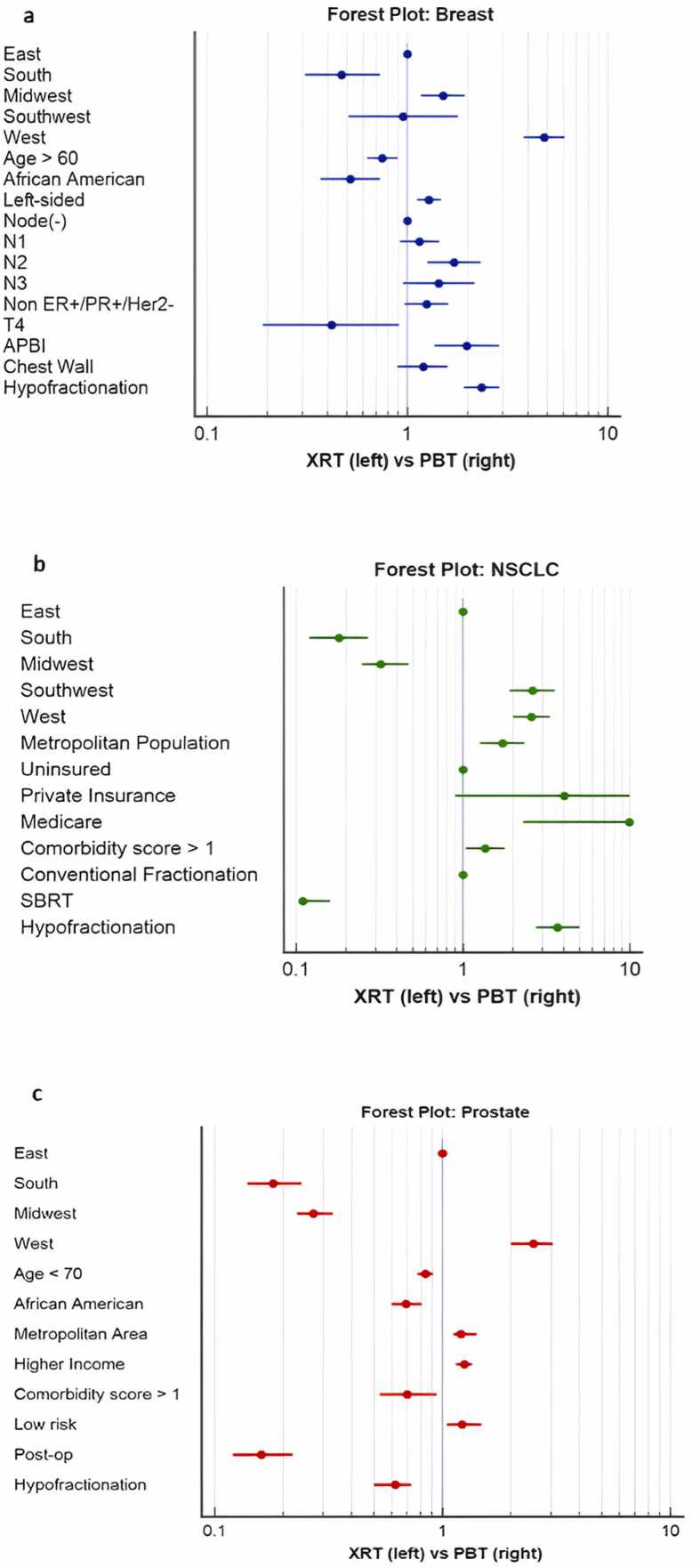
In total, 231 facilities with access to proton centers accounted for 168 323 breast, 39 975 lung, and 77 297 prostate cancer patients treated definitively. Proton beam therapy was used in 0.5%, 1.5%, and 8.9% of breast, lung, and prostate cases. Proton beam therapy was correlated with a farther distance traveled and longer start time from diagnosis for each site ( < .05).For breast, demographic correlates of PBT were treatment in the west coast (odds ratio [OR] = 4.81), age <60 (OR = 1.25), white race (OR = 1.94), and metropolitan area (OR = 1.58). Left-sided cancers (OR = 1.28), N2 (OR = 1.71), non-ER+/PR+/Her2Neu- cancers (OR = 1.24), accelerated partial breast irradiation (OR = 1.98), and hypofractionation (OR = 2.35) were predictors of PBT.For nonsmall cell cancer, demographic correlates of PBT were treatment in the south (OR = 2.6), metropolitan area (OR = 1.72), and Medicare insurance (OR = 1.64). Higher comorbid score (OR = 1.36), later year treated (OR = 3.16), and hypofractionation (not SBRT) (OR = 3.7) were predictors of PBT.For prostate, correlates of PBT were treatment in the west coast (OR = 2.48), age <70 (OR = 1.19), white race (OR = 1.41), metropolitan area (OR = 1.25), higher income/education (OR = 1.25), and treatment at an academic center (OR = 33.94). Lower comorbidity score (OR = 1.42), later year treated (OR = 1.37), low-risk disease (OR = 1.45), definitive compared to postoperative (OR = 6.10), and conventional fractionation (OR = 1.64) were predictors of PBT.
Even for facilities with established referrals to proton centers, PBT utilization was low; socioeconomic status was potentially a factor. Proton beam therapy was more often used with left-sided breast and low-risk prostate cancers, without a clear clinical pattern in lung cancer.
报告相较于光子治疗,更有可能接受质子束治疗(PBT)的患者的人口统计学和临床特征,这些患者来自可接入质子中心的机构。
我们利用国家癌症数据库,确定了2004年至2015年间可接入PBT的机构,并比较了光子和PBT在乳腺癌、前列腺癌和非小细胞癌的人口统计学和临床情况中的相对使用情况。
总共有231家可接入质子中心的机构,共确诊治疗了168323例乳腺癌患者、39975例肺癌患者和77297例前列腺癌患者。质子束治疗在乳腺癌、肺癌和前列腺癌病例中的使用比例分别为0.5%、1.5%和8.9%。质子束治疗与每个部位患者从诊断到治疗的行程更远、开始时间更长相关(P<0.05)。对于乳腺癌,PBT的人口统计学相关因素包括在西海岸接受治疗(优势比[OR]=4.81)、年龄<60岁(OR=1.25)、白人种族(OR=1.94)和大都市区(OR=1.58)。左侧癌症(OR=1.28)、N2期(OR=1.71)、非雌激素受体阳性/孕激素受体阳性/人表皮生长因子受体2阴性癌症(OR=1.24)、加速部分乳腺照射(OR=1.98)和低分割放疗(OR=2.35)是PBT的预测因素。对于非小细胞癌,PBT的人口统计学相关因素包括在南部接受治疗(OR=2.6)、大都市区(OR=1.72)和医疗保险(OR=1.64)。较高的合并症评分(OR=1.36)、较晚治疗年份(OR=3.16)和低分割放疗(非立体定向放疗)(OR=3.7)是PBT的预测因素。对于前列腺癌,PBT的相关因素包括在西海岸接受治疗(OR=2.48)、年龄<70岁(OR=1.19)、白人种族(OR=1.41)、大都市区(OR=1.25)、较高的收入/教育水平(OR=1.25)以及在学术中心接受治疗(OR=33.94)。较低的合并症评分(OR=1.42)、较晚治疗年份(OR=1.37)、低风险疾病(OR=1.45)、与术后治疗相比的根治性治疗(OR=6.10)以及常规分割放疗(OR=1.64)是PBT的预测因素。
即使对于已建立质子中心转诊的机构,PBT的利用率也很低;社会经济地位可能是一个因素。质子束治疗更常用于左侧乳腺癌和低风险前列腺癌,在肺癌中没有明确的临床模式。