Chowdhary Mudit, Lee Anna, Gao Sarah, Wang Dian, Barry Parul N, Diaz Roberto, Bagadiya Neeti R, Park Henry S, Yu James B, Wilson Lynn D, Moran Meena S, Higgins Susan A, Knowlton Christin A, Patel Kirtesh R
Department of Radiation Oncology, Rush University Medical Center, Chicago, IL, United States.
Department of Radiation Oncology, SUNY Downstate Medical Center, Brooklyn, NY, United States.
Front Oncol. 2019 Jan 14;8:678. doi: 10.3389/fonc.2018.00678. eCollection 2018.
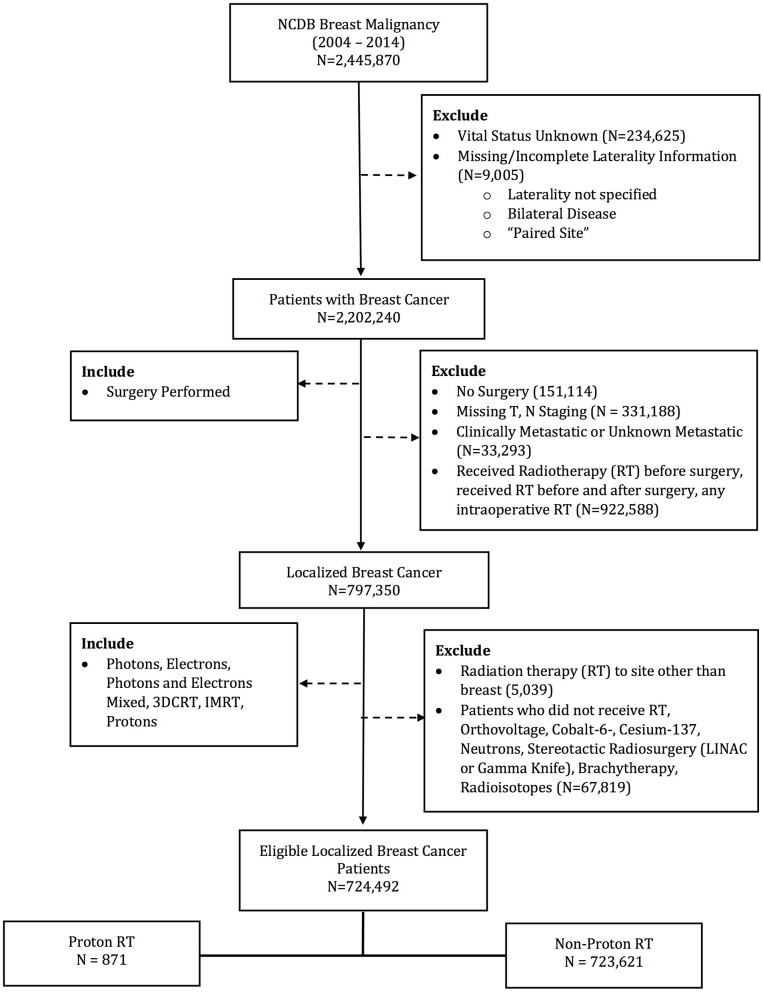
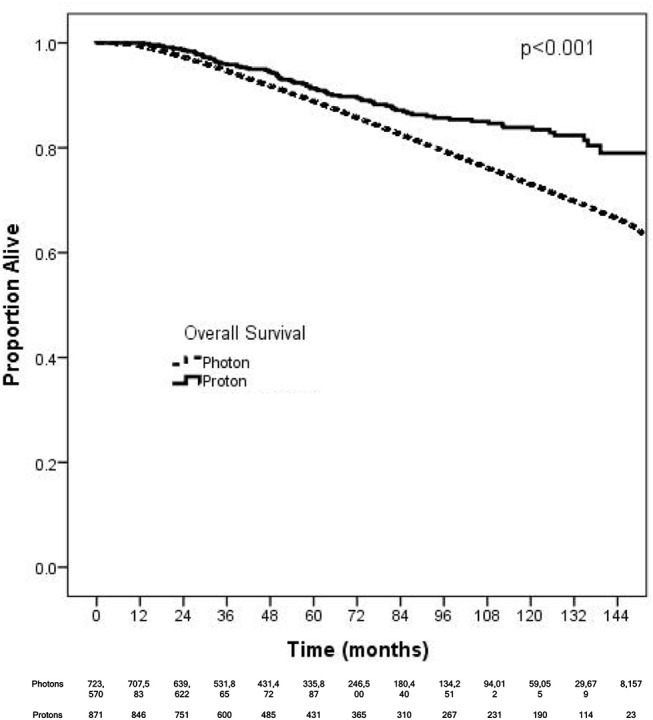
Limited data exists demonstrating the clinical benefit of proton radiotherapy (PRT) in breast cancer. Using the National Cancer Database, we evaluated predictors associated with PRT use for patients with breast cancer. An exploratory analysis also investigates the impact of PRT on overall survival (OS). Patients with non-metastatic breast cancer treated with adjuvant radiotherapy from 2004 to 2014 were identified. Patients were stratified based on receipt of PRT or non-PRT (i.e., photons ± electrons). A logistic regression model was used to determine predictors for PRT utilization. For OS, Multivariable analysis (MVA) was performed using Cox proportional hazard model. A total of 724,492 patients were identified: 871 received PRT and 723,621 received non-PRT. 58.3% of the PRT patients were group stage 0-1. Median follow-up time was 62.2 months. On multivariate logistic analysis, the following factors were found to be significant for receipt of PRT (all < 0.05): academic facility (odds ratio [OR] = 2.50), South (OR = 2.01) and West location (OR = 12.43), left-sided (OR = 1.21), ER-positive (OR = 1.59), and mastectomy (OR = 1.47); pT2-T4 disease predicted for decrease use (OR = 0.79). PRT was not associated with OS on MVA for all patients: Hazard Ratio: 0.85, = 0.168. PRT remained not significant on MVA after stratifying for subsets likely associated with higher heart radiation doses, including: left-sided ( = 0.140), inner-quadrant ( = 0.173), mastectomy ( = 0.095), node positivity ( = 0.680), N2-N3 disease ( = 0.880), and lymph node irradiation (LNI) ( = 0.767). Receipt of PRT was associated with left-sided, ER+ tumors, mastectomy, South and West location, and academic facilities, but not higher group stages or LNI. PRT was not associated with OS, including in subsets likely at risk for higher heart doses. Further studies are required to determine non-OS benefits of PRT. In the interim, given the high cost of protons, only well-selected patients should receive PRT unless enrolled on a clinical trial.
现有数据有限,难以证明质子放射治疗(PRT)对乳腺癌的临床益处。我们利用国家癌症数据库,评估了乳腺癌患者接受PRT治疗的相关预测因素。一项探索性分析还研究了PRT对总生存期(OS)的影响。我们确定了2004年至2014年接受辅助放疗的非转移性乳腺癌患者。根据是否接受PRT或非PRT(即光子±电子)对患者进行分层。使用逻辑回归模型确定PRT使用的预测因素。对于OS,使用Cox比例风险模型进行多变量分析(MVA)。共确定了724,492例患者:871例接受了PRT,723,621例接受了非PRT。接受PRT的患者中58.3%为0-1期。中位随访时间为62.2个月。在多变量逻辑分析中,发现以下因素对接受PRT具有显著意义(均P<0.05):学术机构(比值比[OR]=2.50)、南部地区(OR=2.01)和西部地区(OR=12.43)、左侧(OR=1.21)阳性、雌激素受体(ER)阳性(OR=1.59)和乳房切除术(OR=1.47);pT2-T4期疾病预测使用减少(OR=0.79)。在所有患者的MVA中,PRT与OS无关:风险比:0.85,P=0.168。在对可能与较高心脏辐射剂量相关的亚组进行分层后,PRT在MVA中仍无显著意义,这些亚组包括:左侧(P=0.140)、内象限(P=0.173)、乳房切除术(P=0.095)、淋巴结阳性(P=0.680)、N2-N3期疾病(P=0.880)和淋巴结照射(LNI)(P=0.767)。接受PRT与左侧、ER+肿瘤、乳房切除术、南部和西部地区以及学术机构有关,但与较高分期或LNI无关。PRT与OS无关,包括在可能有较高心脏剂量风险的亚组中。需要进一步研究以确定PRT的非OS益处。在此期间,鉴于质子治疗成本高昂,除非参加临床试验,只有精心挑选的患者才应接受PRT。