Department of Hematology and Oncology Graduate School of Medicine, Kyoto University, 54, Kyoto, Kawaramachi, Shogoin, Sakyoku, 606-8507, Japan.
Kyoto Innovation Center for Next Generation Clinical Trials and iPS Cell Therapy, Kyoto University Hospital, Kyoto, Japan.
Cancer Immunol Immunother. 2024 May 17;73(7):135. doi: 10.1007/s00262-024-03711-8.
Isatuximab, an anti-CD38 antibody, has been widely used in treatments for patients with relapsed/refractory multiple myeloma (MM). Despite its high efficacy, not all patients achieve a lasting therapeutic response with isatuximab.
We tried to identify biomarkers to predict the effectiveness of isatuximab by focusing on the host's immune status before treatment.
We retrospectively analyzed the cases of 134 relapsed/refractory MM patients in the Kansai Myeloma Forum database who had received only a first isatuximab treatment.
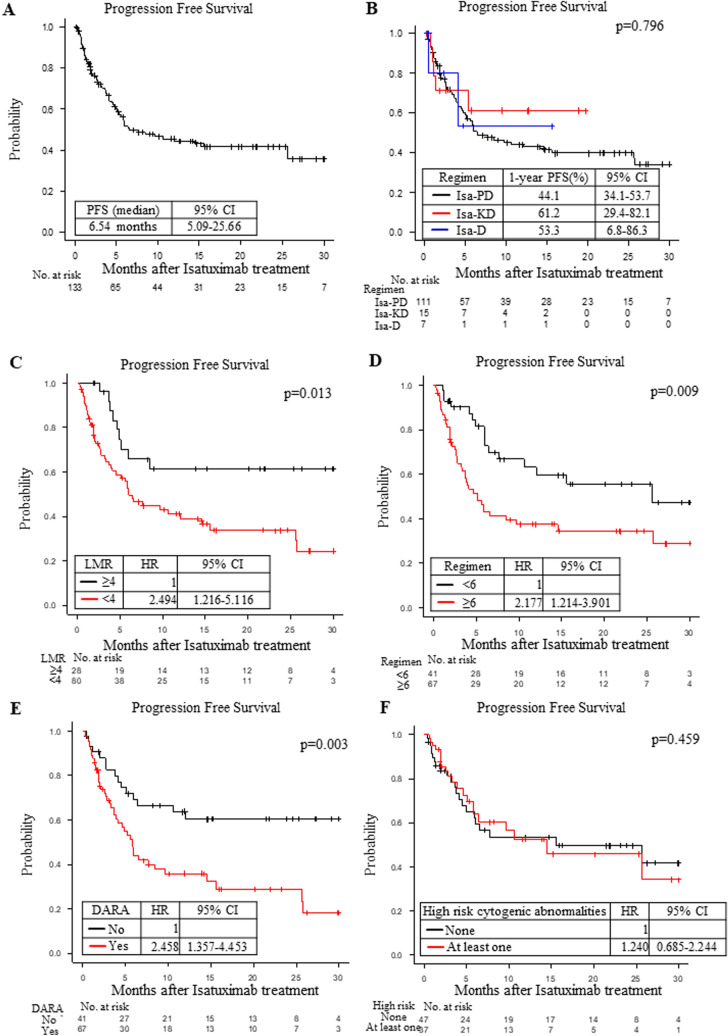
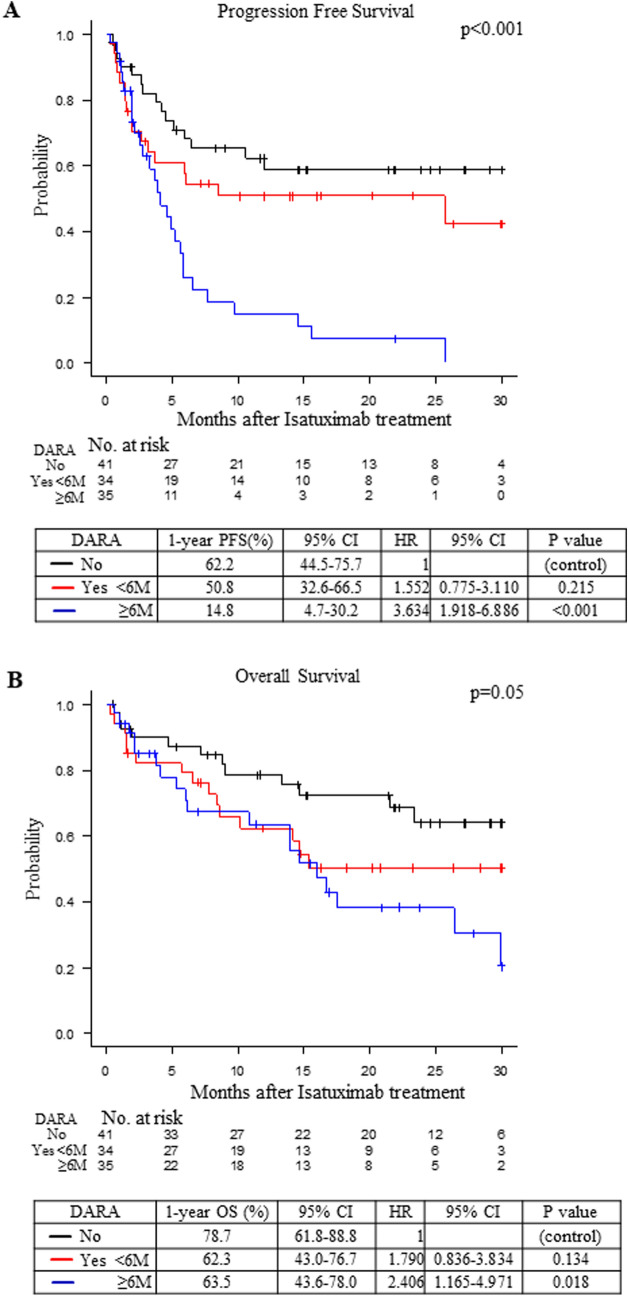
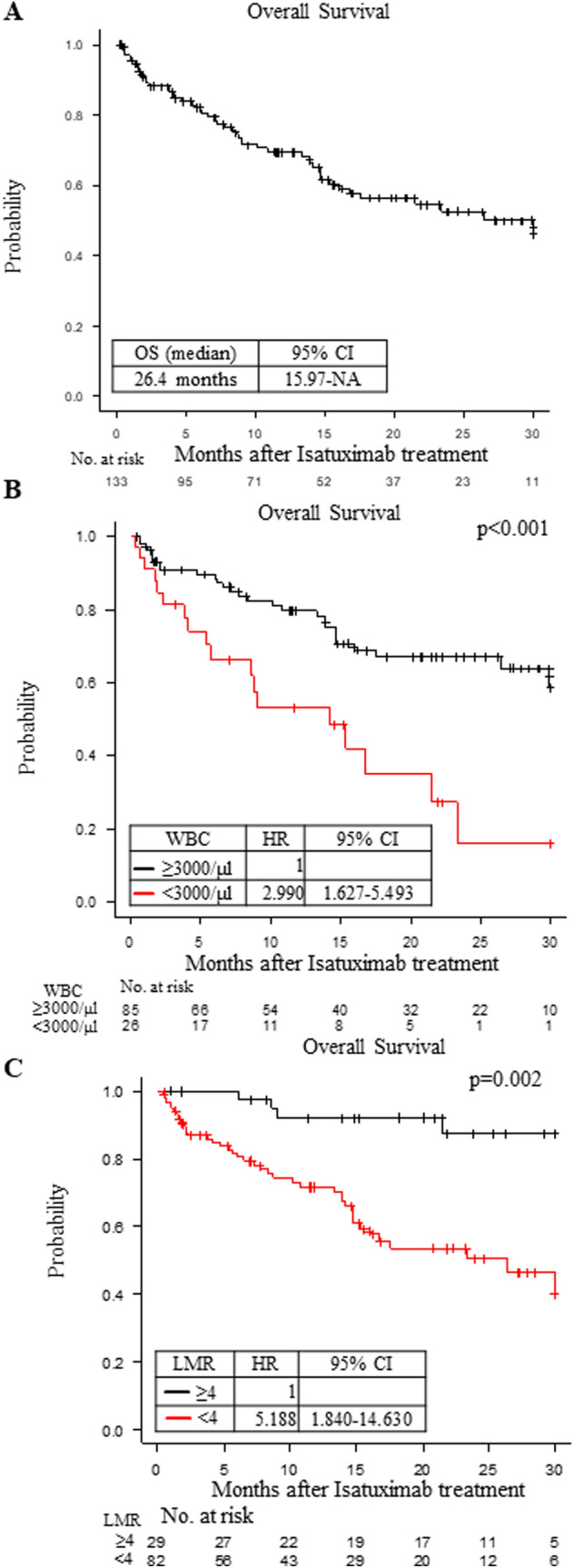
Among the 134 patients, an isatuximab, pomalidomide and dexamethasone (Isa-PD) regimen, isatuximab, carfilzomib and dexamethasone (Isa-KD) regimen and isatuximab and/or dexamethasone (Isa-D) regimen were used in 112, 15 and 7 patients, respectively. The median age at treatment, number of prior treatment regimens, and progression-free survival (PFS) were 71, 6, and 6.54 months, respectively. Multivariate analysis showed that the PFS under the Isa-PD regimen was longer in patients with higher lymphocyte/monocyte ratio (LMR ≥ 4), fewer prior treatment regimens (< 6), and no use of prior daratumumab treatment. The OS under the Isa-PD regimen was longer in patients with higher white blood cell counts (WBC counts ≥ 3000/μL) and higher LMR. The PFS under the Isa-D regimen was longer in patients with fewer prior treatment regimens in univariate analysis, but no parameters were correlated with PFS/OS under the Isa-KD regimen.
We found that the patients with higher LMR (≥ 4) could obtain longer PFS and OS under the Isa-PD regimen. Other cohort studies of isatuximab treatment might be necessary to substantiate our results.
抗 CD38 抗体伊沙妥昔单抗已广泛用于治疗复发/难治性多发性骨髓瘤(MM)患者。尽管疗效显著,但并非所有患者使用伊沙妥昔单抗都能获得持久的治疗反应。
我们试图通过关注治疗前宿主的免疫状态来确定预测伊沙妥昔单抗疗效的生物标志物。
我们回顾性分析了关西骨髓瘤论坛数据库中 134 例仅接受首次伊沙妥昔单抗治疗的复发/难治性 MM 患者的病例。
在 134 例患者中,112 例患者使用伊沙妥昔单抗、泊马度胺和地塞米松(Isa-PD)方案,15 例患者使用伊沙妥昔单抗、卡非佐米和地塞米松(Isa-KD)方案,7 例患者使用伊沙妥昔单抗和/或地塞米松(Isa-D)方案。治疗时的中位年龄、先前治疗方案的数量和无进展生存期(PFS)分别为 71 岁、6 个和 6.54 个月。多变量分析显示,在 LMR≥4(淋巴细胞/单核细胞比值)较高、先前治疗方案较少(<6 个)且未使用先前达雷妥尤单抗治疗的患者中,Isa-PD 方案的 PFS 更长。在白细胞计数(WBC 计数≥3000/μL)和 LMR 较高的患者中,Isa-PD 方案的 OS 更长。在单变量分析中,Isa-D 方案的 PFS 在先前治疗方案较少的患者中更长,但 Isa-KD 方案的任何参数均与 PFS/OS 无关。
我们发现,在 Isa-PD 方案中,较高的 LMR(≥4)患者可以获得更长的 PFS 和 OS。可能需要进行其他伊沙妥昔单抗治疗的队列研究来证实我们的结果。