Departments of Nuclear Medicine, Saarland University - Medical Center, Kirrberger Str. 100, Geb. 50, 66421, Homburg, Germany.
Spencer-Fontayne Corporation, Jersey City, NJ, USA.
Sci Rep. 2024 May 17;14(1):11271. doi: 10.1038/s41598-024-61961-z.
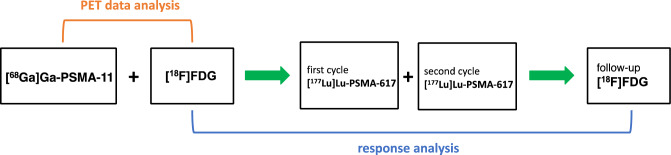
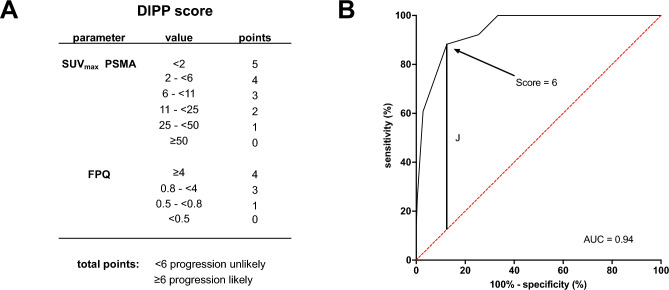
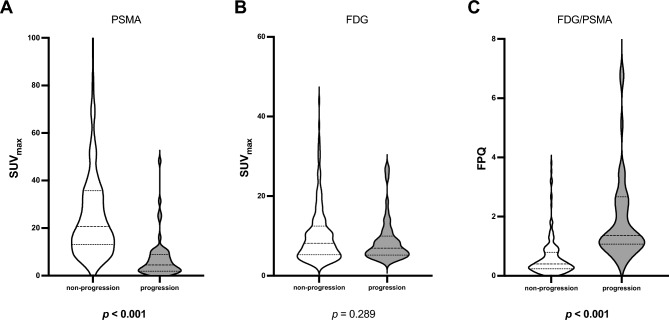
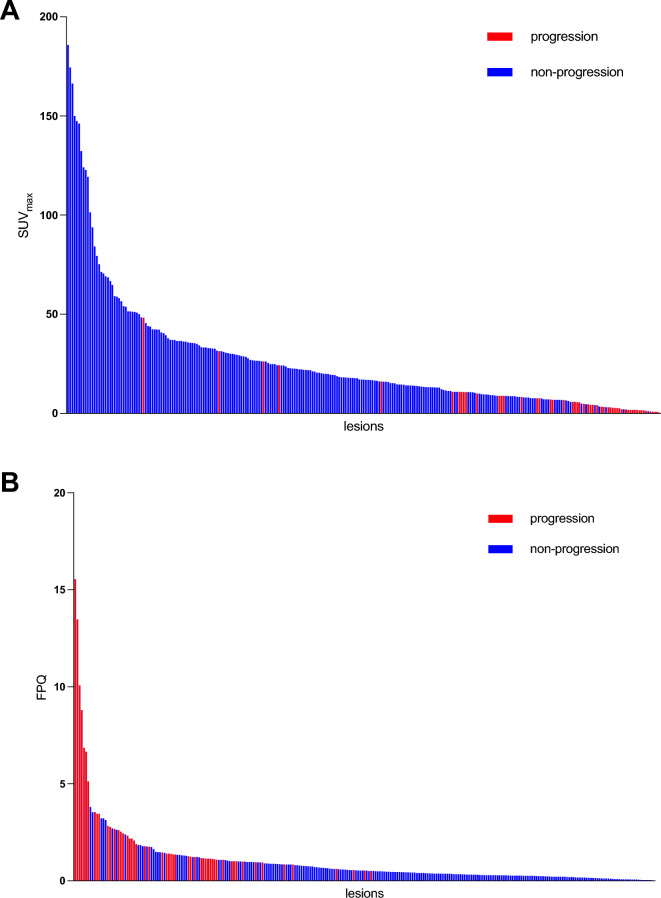
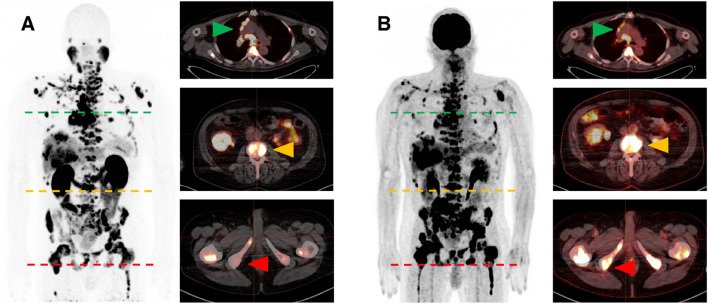
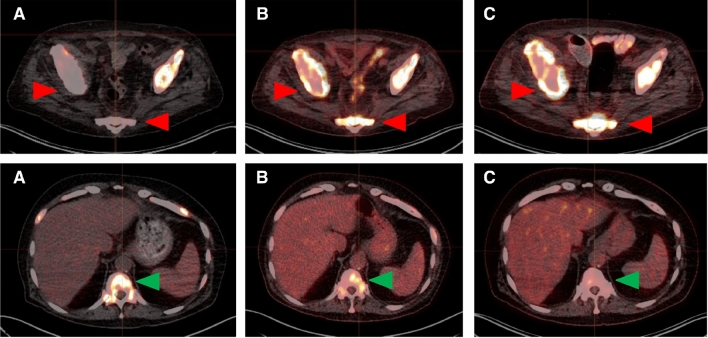
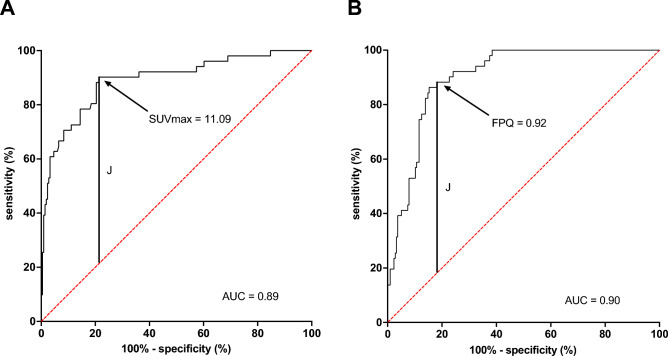
Candidates for prostate-specific membrane antigen (PSMA)-targeted radioligand therapy (RLT) of metastatic castration-resistant prostate cancer (mCRPC) frequently have "mismatch" lesions with pronounced 18-fluorodeoxyglucose ([F]FDG) but attenuated PSMA ligand uptake on positron emission tomography (PET). However, no quantitative criteria yet exist to identify mismatch lesions and predict their response to RLT. To define such criteria, we retrospectively analyzed 267 randomly-selected glucometabolic mCRPC metastases from 22 patients. On baseline PET, we determined [F]FDG and [Ga]Ga-PSMA-11 maximum standardized uptake value (SUV), and calculated the [F]FDG SUV/[Ga]Ga-PSMA-11 SUV quotient (FPQ). From follow-up [F]FDG PET after two lutetium-177-PSMA-617 RLT cycles, we evaluated the treatment response and categorized the lesions into three subgroups (partial remission, stable disease, progression) based on change in [F]FDG SUV. Lastly, we compared the baseline PET variables in progressing versus non-progressing lesions. Variables differing significantly, and a score incorporating them, were assessed via receiver operator characteristic (ROC) curve analysis, regarding ability to predict lesional progression, with area under the curve (AUC) as metric. Cut-offs with optimal sensitivity and specificity were determined using the maximum value of Youden's index. Fifty-one of 267 lesions (19.1%) progressed, 102/267 (38.2%) manifested stable disease, and 114/267 (42.7%) partially responded after two RLT cycles. At baseline, median [Ga]Ga-PSMA-11 SUV was significantly lower (p < 0.001), median FPQ significantly higher (p < 0.001), and median [F]FDG SUV similar in progressing versus non-progressing lesions. [Ga]Ga-PSMA-11 SUV and FPQ showed predictive power regarding progression (AUCs: 0.89, 0.90). An introduced clinical score combining both further improved predictive performance (AUC: 0.94). Optimal cut-offs to foretell progression were: [Ga]Ga-PSMA-11 SUV < 11.09 (88.2% sensitivity, 81.9% specificity), FPQ ≥ 0.92 (90.2% sensitivity, 78.7% specificity), clinical score ≥ 6/9 points (88.2% sensitivity, 87.5% specificity). At baseline, a low [ Ga]Ga-PSMA-11 SUV and a high FPQ predict early lesional progression under RLT; [F]FDG SUV does not. A score combining [ Ga]Ga-PSMA-11 SUV and FPQ predicts early lesional progression even more effectively and might therefore be useful to quantitatively identify mismatch lesions.
候选者前列腺特异性膜抗原(PSMA)-靶向放射性配体治疗(RLT)转移性去势抵抗性前列腺癌(mCRPC)经常有“不匹配”的病变,表现为明显的 18-氟脱氧葡萄糖([F]FDG)摄取,但 PSMA 配体摄取减弱在正电子发射断层扫描(PET)上。然而,目前还没有定量标准来识别不匹配的病变并预测它们对 RLT 的反应。为了定义这些标准,我们回顾性分析了 22 名患者的 267 个随机选择的葡萄糖代谢 mCRPC 转移灶。在基线 PET 上,我们确定了[F]FDG 和[Ga]Ga-PSMA-11 的最大标准化摄取值(SUV),并计算了[F]FDG SUV/[Ga]Ga-PSMA-11 SUV 比值(FPQ)。从两次镥-177-PSMA-617 RLT 循环后的后续[F]FDG PET 中,我们评估了治疗反应,并根据[F]FDG SUV 的变化将病变分为三组(部分缓解、稳定疾病、进展)。最后,我们比较了进展性和非进展性病变的基线 PET 变量。通过接收者操作特征(ROC)曲线分析,对差异显著的变量及其包含的评分进行评估,以评估其预测病变进展的能力,以曲线下面积(AUC)为指标。使用 Youden 指数的最大值确定具有最佳灵敏度和特异性的截止值。267 个病变中有 51 个(19.1%)进展,102/267(38.2%)表现为稳定疾病,114/267(42.7%)在两次 RLT 循环后部分缓解。在基线时,[Ga]Ga-PSMA-11 SUV 明显较低(p < 0.001),FPQ 明显较高(p < 0.001),进展性和非进展性病变的[F]FDG SUV 相似。[Ga]Ga-PSMA-11 SUV 和 FPQ 对进展具有预测能力(AUC:0.89,0.90)。引入的联合两种方法的临床评分进一步提高了预测性能(AUC:0.94)。预测进展的最佳截止值为:[Ga]Ga-PSMA-11 SUV < 11.09(88.2%的敏感性,81.9%的特异性),FPQ ≥ 0.92(90.2%的敏感性,78.7%的特异性),临床评分≥6/9 分(88.2%的敏感性,87.5%的特异性)。在基线时,低[Ga]Ga-PSMA-11 SUV 和高 FPQ 预测 RLT 下早期病变进展;[F]FDG SUV 则不然。联合[Ga]Ga-PSMA-11 SUV 和 FPQ 的评分可以更有效地预测早期病变进展,因此可能有助于定量识别不匹配的病变。