Division of Hematology & Medical Oncology, Meyer Cancer Center, Weill Cornell Medicine, New York, NY.
Division of Hematology and Medical Oncology, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY.
Blood Adv. 2024 Aug 13;8(15):3859-3869. doi: 10.1182/bloodadvances.2023012470.
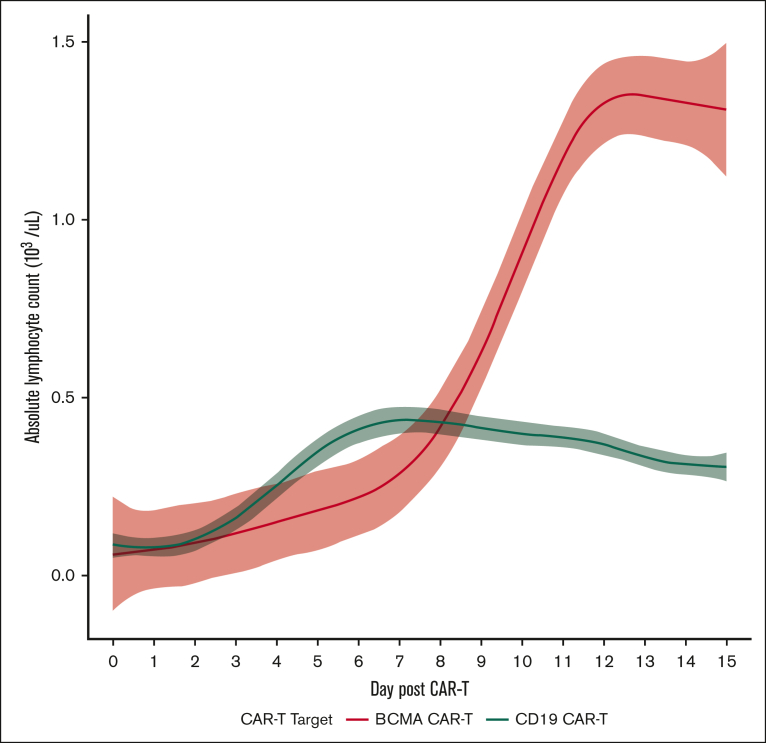
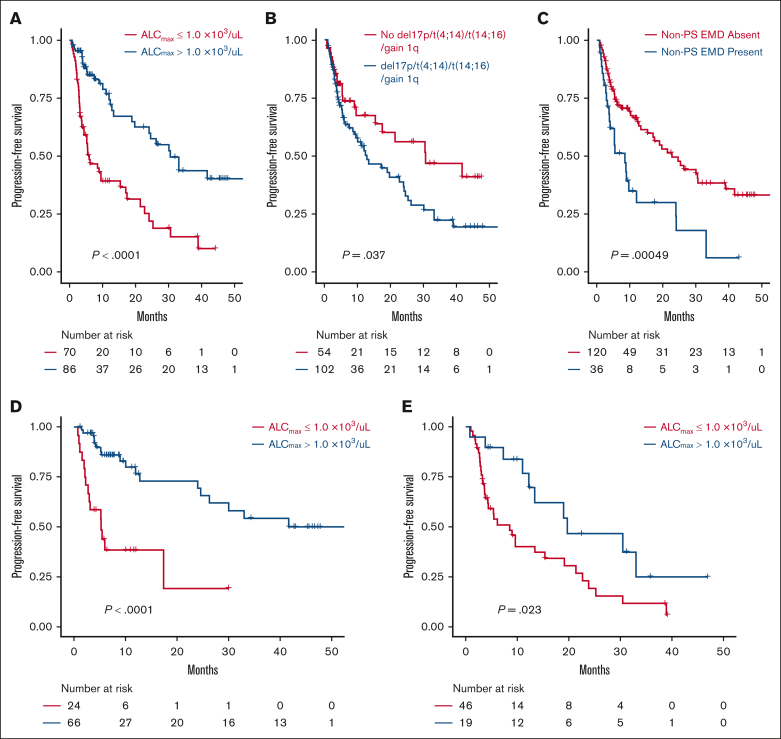
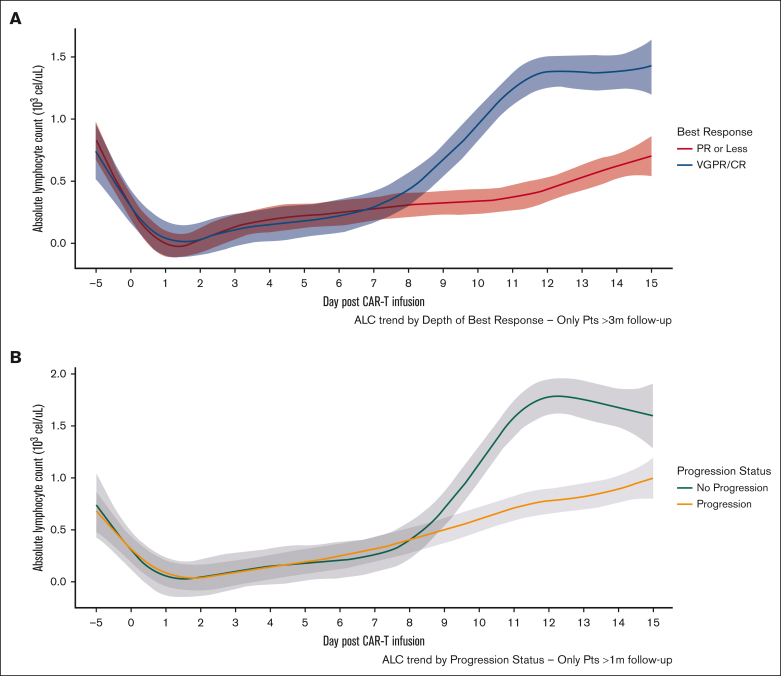
B-cell maturation antigen (BCMA)-targeting chimeric antigen receptor T cells (CAR-Ts) used in multiple myeloma (MM) are rapidly becoming a mainstay in the treatment of relapsed/refractory (R/R) disease, and CAR-T expansion after infusion has been shown to inform depth and duration of response (DoR), but measuring this process remains investigational. This multicenter study describes the kinetics and prognostic impact of absolute lymphocyte count (ALC) in the first 15 days after CAR-T infusion in 156 patients with relapsed MM treated with the BCMA-targeting agents ciltacabtagene autoleucel and idecabtagene vicleucel. Patients with higher maximum ALC (ALCmax) had better depth of response, progression-free survival (PFS), and DoR. Patients with ALCmax >1.0 × 103/μL had a superior PFS (30.5 months vs 6 months; P < .001) compared with those with ≤1.0 × 103/μL, whereas patients with ALCmax ≤0.5 × 103/μL represent a high-risk group with early disease progression and short PFS (hazard ratio, 3.4; 95% confidence interval, 2-5.8; P < .001). In multivariate analysis, ALCmax >1.0 × 103/μL and nonparaskeletal extramedullary disease were the only independent predictors of PFS and DoR after accounting for international staging systemic staging, age, CAR-T product, high-risk cytogenetics, and the number of previous lines. Moreover, our flow cytometry data suggest that ALC is a surrogate for BCMA CAR-T expansion and can be used as an accessible prognostic marker. We report, to our knowledge, for the first time the association of ALC after BCMA CAR-T infusion with clinical outcomes and its utility in predicting response in patients with R/R MM.
B 细胞成熟抗原 (BCMA)- 靶向嵌合抗原受体 T 细胞 (CAR-T) 已广泛用于多发性骨髓瘤 (MM) 的治疗,成为复发性/难治性 (R/R) 疾病的主要治疗手段。CAR-T 输注后的扩增情况与反应深度和持续时间 (DoR) 相关,但目前仍在研究如何对其进行测量。本多中心研究描述了 156 例接受 BCMA 靶向药物 cilta-cabtagene autoleucel 和 idecabtagene vicleucel 治疗的复发性 MM 患者在 CAR-T 输注后 15 天内绝对淋巴细胞计数 (ALC) 的动力学及其对预后的影响。最大 ALC (ALCmax) 较高的患者反应深度、无进展生存期 (PFS) 和 DoR 更好。ALCmax >1.0×103/μL 的患者的 PFS 优于 ALCmax ≤1.0×103/μL 的患者(30.5 个月 vs 6 个月;P <.001),而 ALCmax ≤0.5×103/μL 的患者属于高危组,疾病进展较早,PFS 较短(风险比,3.4;95%置信区间,2-5.8;P <.001)。多变量分析表明,ALCmax >1.0×103/μL 和非骨骼外髓外疾病是 PFS 和 DoR 的唯一独立预测因素,在考虑国际分期系统、年龄、CAR-T 产品、高危细胞遗传学和先前治疗线数后。此外,我们的流式细胞术数据表明,ALC 是 BCMA CAR-T 扩增的替代物,可用作可及的预后标志物。据我们所知,这是首次报道 BCMA CAR-T 输注后 ALC 与临床结局的相关性及其在预测 R/R MM 患者反应中的应用。