Department of Infectious Diseases and Clinical Microbiology, Faculty of Medicine, Akdeniz University, Antalya, Turkey.
Department of Internal Medicine, Division of Nephrology, Faculty of Medicine, Akdeniz University, Antalya, Turkey.
BMC Infect Dis. 2024 May 24;24(1):526. doi: 10.1186/s12879-024-09413-x.
The recently used pan-immune-inflammation value (PIV) has not been adequately studied as a predictive marker for mortality in immunosuppressed patients. The aim of this study was to evaluate the usefulness of baseline PIV level as a predictor of 30-day mortality in solid organ transplant (SOT) recipients with gram negative bloodstream infections (GN-BSI).
This retrospective, cross-sectional study was conducted between January 1, 2019, and December 31, 2022, in 1104 SOT recipients. During the study period, 118 GN-BSI were recorded in 113 patients. Clinical, epidemiological, and laboratory data were collected, and mortality rates (30-day and all-cause) were recorded.
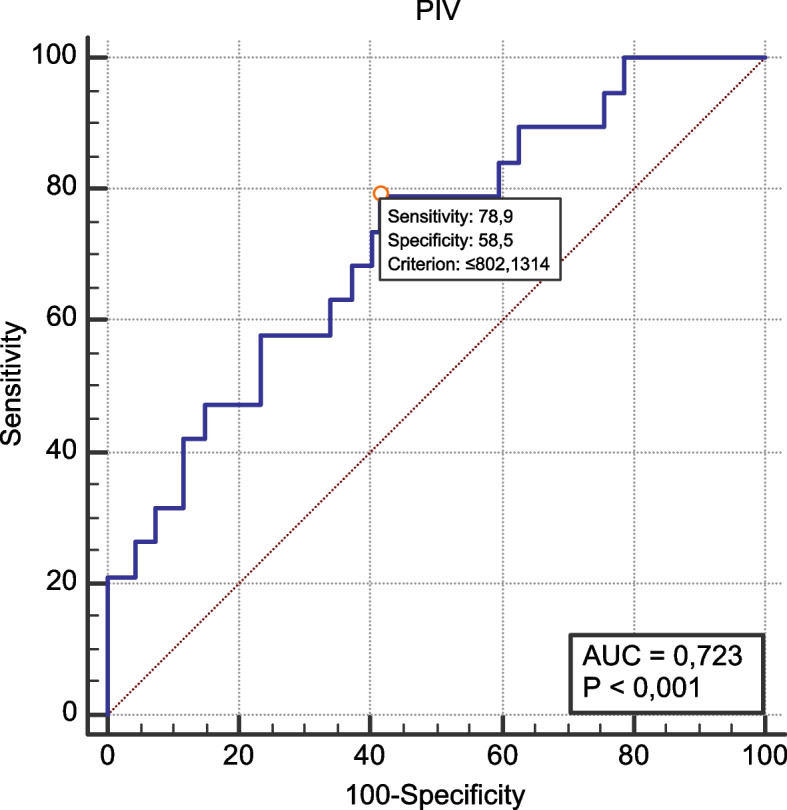
The 113 recipients had a median age of 50 years [interquartile range (IQR) 37.5-61.5 years] with a male predominance (n = 72, 63.7%). The three most common microorganisms were as follows: 46 isolates (38.9%) of Escherichia coli, 41 (34.7%) of Klebsiella pneumoniae, and 12 (10.2%) of Acinetobacter baumannii. In 44.9% and 35.6% of the isolates, production of extended-spectrum beta-lactamases and carbapenem resistance were detected, respectively. The incidence of carbapenem-resistant GN-BSI was higher in liver recipients than in renal recipients (n = 27, 69.2% vs n = 13, 17.6%, p < 0.001). All-cause and 30-day mortality rates after GN-BSI were 26.5% (n = 30), and 16.8% (n = 19), respectively. In the group with GN-BSI-related 30-day mortality, the median PIV level was significantly lower (327.3, IQR 64.8-795.4 vs. 1049.6, IQR 338.6-2177.1; p = 0.002). The binary logistic regression analysis identified low PIV level [hazard ratio (HR) = 0.93, 95% confidence interval (CI) 0.86-0.99; p = 0.04], and increased age (HR = 1.05, 95% CI 1.01-1.09; p = 0.002) as factors associated with 30-day mortality. The receiver operating characteristic analysis revealed that PIV could determine the GN-BSI-related 30-day mortality with area under curve (AUC): 0.723, 95% CI 0.597-0.848, p = 0.0005.
PIV is a simple and inexpensive biomarker that can be used to estimate mortality in immunosuppressed patients, but the results need to be interpreted carefully.
最近使用的泛免疫炎症值(PIV)作为预测免疫抑制患者死亡率的指标尚未得到充分研究。本研究旨在评估基线 PIV 水平作为预测革兰氏阴性菌血流感染(GN-BSI)的实体器官移植(SOT)受者 30 天死亡率的有用性。
本回顾性、横断面研究于 2019 年 1 月 1 日至 2022 年 12 月 31 日在 1104 名 SOT 受者中进行。研究期间,在 113 名患者中记录了 118 例 GN-BSI。收集了临床、流行病学和实验室数据,并记录了死亡率(30 天和全因)。
113 名受者的中位年龄为 50 岁[四分位距(IQR)37.5-61.5 岁],以男性为主(n=72,63.7%)。最常见的三种微生物如下:46 株(38.9%)大肠埃希菌、41 株(34.7%)肺炎克雷伯菌和 12 株(10.2%)鲍曼不动杆菌。在 44.9%和 35.6%的分离株中分别检测到产超广谱β-内酰胺酶和碳青霉烯类耐药。与肾移植受者相比,肝移植受者中发生耐碳青霉烯类 GN-BSI 的比例更高(n=27,69.2% vs n=13,17.6%,p<0.001)。GN-BSI 后全因和 30 天死亡率分别为 26.5%(n=30)和 16.8%(n=19)。在与 GN-BSI 相关的 30 天死亡率组中,中位 PIV 水平明显降低(327.3,IQR 64.8-795.4 与 1049.6,IQR 338.6-2177.1;p=0.002)。二元逻辑回归分析确定低 PIV 水平[危险比(HR)=0.93,95%置信区间(CI)0.86-0.99;p=0.04]和年龄增加(HR=1.05,95%CI 1.01-1.09;p=0.002)是与 30 天死亡率相关的因素。受试者工作特征分析显示,PIV 可通过曲线下面积(AUC)来确定与 GN-BSI 相关的 30 天死亡率:0.723,95%CI 0.597-0.848,p=0.0005。
PIV 是一种简单且廉价的生物标志物,可用于评估免疫抑制患者的死亡率,但结果需要谨慎解释。