Breast Unit, Kliniken Essen Mitte, Essen, Germany.
Department of Gynecology with Breast Center, Charité - Universitätsmedizin Berlin, Berlin, Germany.
BMC Cancer. 2024 May 24;24(1):641. doi: 10.1186/s12885-024-12179-9.
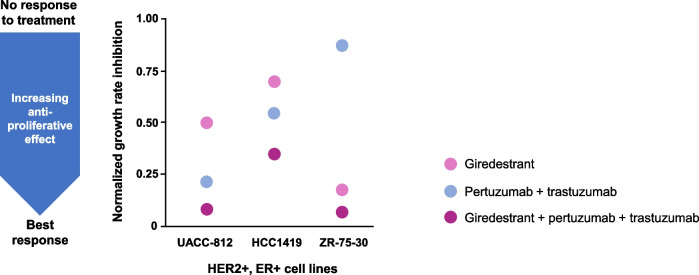
HER2-positive, estrogen receptor-positive breast cancer (HER2+, ER+ BC) is a distinct disease subtype associated with inferior response to chemotherapy plus HER2-targeted therapy compared with HER2+, ER-negative BC. Bi-directional crosstalk leads to cooperation of the HER2 and ER pathways that may drive treatment resistance; thus, simultaneous co-targeting may optimize treatment impact and survival outcomes in patients with HER2+, ER+ BC. First-line (1L) treatment for patients with HER2+ metastatic BC (mBC) is pertuzumab, trastuzumab, and taxane chemotherapy. In clinical practice, dual HER2 blockade plus a fixed number of chemotherapy cycles are given as induction therapy to maximize tumor response, with subsequent HER2-targeted maintenance treatment given as a more tolerable regimen for long-term disease control. For patients whose tumors co-express ER, maintenance endocrine therapy (ET) can be added, but uptake varies due to lack of data from randomized clinical trials investigating the superiority of maintenance ET plus dual HER2 blockade versus dual HER2 blockade alone. Giredestrant, a novel oral selective ER antagonist and degrader, shows promising clinical activity and manageable safety across phase I-II trials of patients with ER+, HER2-negative BC, with therapeutic potential in those with HER2 co-expression.
This phase III, randomized, open-label, two-arm study aims to recruit 812 patients with HER2+, ER+ locally advanced (LA)/mBC into the induction phase (fixed-dose combination of pertuzumab and trastuzumab for subcutaneous injection [PH FDC SC] plus a taxane) to enable 730 patients to be randomized 1:1 to the maintenance phase (giredestrant plus PH FDC SC or PH FDC SC [plus optional ET]), stratified by disease site (visceral versus non-visceral), type of LA/metastatic presentation (de novo versus recurrent), best overall response to induction therapy (partial/complete response versus stable disease), and intent to give ET (yes versus no). The primary endpoint is investigator-assessed progression-free survival. Secondary endpoints include overall survival, objective response rate, clinical benefit rate, duration of response, safety, and patient-reported outcomes.
heredERA BC will address whether giredestrant plus dual HER2 blockade is superior to dual HER2 blockade alone, to inform the use of this combination in clinical practice for maintenance 1L treatment of patients with HER2+, ER+ LA/mBC.
ClinicalTrials.gov, NCT05296798; registered on March 25, 2022. Protocol version 3.0 (November 18, 2022).
F. Hoffmann-La Roche Ltd, Grenzacherstrasse 124 4070, Basel, Switzerland.
人表皮生长因子受体 2(HER2)阳性、雌激素受体阳性(HER2+、ER+)乳腺癌是一种独特的疾病亚型,与 HER2+、ER-阴性乳腺癌相比,其对化疗联合 HER2 靶向治疗的反应较差。双向串扰导致 HER2 和 ER 通路的协同作用,可能导致治疗耐药;因此,同时针对这两个通路可能会优化 HER2+、ER+乳腺癌患者的治疗效果和生存结局。HER2 阳性转移性乳腺癌(mBC)患者的一线(1L)治疗是帕妥珠单抗、曲妥珠单抗和紫杉烷化疗。在临床实践中,双 HER2 阻断加一定数量的化疗周期作为诱导治疗,以最大限度地提高肿瘤反应,随后给予更耐受的 HER2 靶向维持治疗,以长期控制疾病。对于肿瘤同时表达 ER 的患者,可以添加维持内分泌治疗(ET),但由于缺乏随机临床试验数据表明维持 ET 加双 HER2 阻断优于单独双 HER2 阻断,因此接受率存在差异。新型口服选择性雌激素受体拮抗剂和降解剂 giredestrant 在 ER+、HER2-阴性乳腺癌的 I 期- II 期试验中显示出有前景的临床活性和可管理的安全性,在 HER2 共表达的患者中具有治疗潜力。
这项 III 期、随机、开放标签、双臂研究旨在招募 812 名 HER2+、ER+局部晚期(LA)/mBC 患者进入诱导期(皮下注射固定剂量组合帕妥珠单抗和曲妥珠单抗[PH FDC SC]加紫杉烷),以使 730 名患者能够 1:1 随机分为维持期(giredestrant 加 PH FDC SC 或 PH FDC SC[加可选 ET]),按疾病部位(内脏与非内脏)、LA/转移性表现类型(初发与复发)、诱导治疗最佳总体反应(部分/完全缓解与稳定疾病)以及是否打算给予 ET(是与否)分层。主要终点是研究者评估的无进展生存期。次要终点包括总生存期、客观缓解率、临床获益率、缓解持续时间、安全性和患者报告的结局。
heredERA BC 将确定 giredestrant 加双 HER2 阻断是否优于单独双 HER2 阻断,为该联合在临床实践中用于维持 1L 治疗 HER2+、ER+ LA/mBC 患者提供依据。
ClinicalTrials.gov,NCT05296798;于 2022 年 3 月 25 日注册。方案版本 3.0(2022 年 11 月 18 日)。
罗氏公司,瑞士巴塞尔格伦策尔大街 124 号 4070。