Department of Biomedical Informatics, University of Utah Spencer Fox Eccles School of Medicine, Salt Lake City, UT 84108, United States.
Department of Internal Medicine, Division of Geriatrics, University of Utah Spencer Fox Eccles School of Medicine, Salt Lake City, UT 84132, United States.
J Am Med Inform Assoc. 2024 Jun 20;31(7):1503-1513. doi: 10.1093/jamia/ocae112.
We sought to (1) characterize the process of diagnosing pneumonia in an emergency department (ED) and (2) examine clinician reactions to a clinician-facing diagnostic discordance feedback tool.
We designed a diagnostic feedback tool, using electronic health record data from ED clinicians' patients to establish concordance or discordance between ED diagnosis, radiology reports, and hospital discharge diagnosis for pneumonia. We conducted semistructured interviews with 11 ED clinicians about pneumonia diagnosis and reactions to the feedback tool. We administered surveys measuring individual differences in mindset beliefs, comfort with feedback, and feedback tool usability. We qualitatively analyzed interview transcripts and descriptively analyzed survey data.
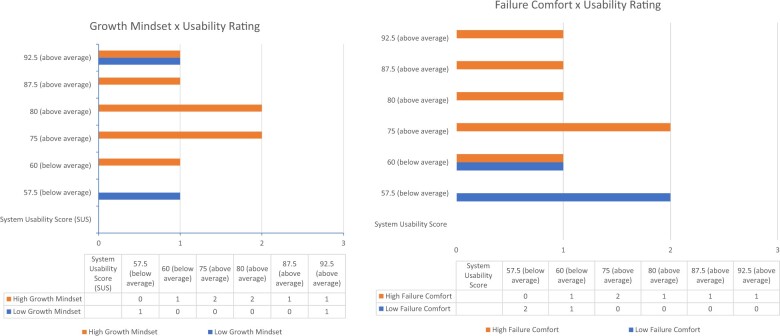
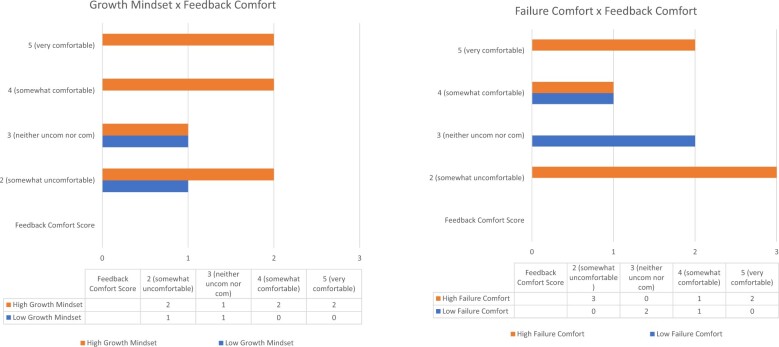
Thematic results revealed: (1) the diagnostic process for pneumonia in the ED is characterized by diagnostic uncertainty and may be secondary to goals to treat and dispose the patient; (2) clinician diagnostic self-evaluation is a fragmented, inconsistent process of case review and follow-up that a feedback tool could fill; (3) the feedback tool was described favorably, with task and normative feedback harnessing clinician values of high-quality patient care and personal excellence; and (4) strong reactions to diagnostic feedback varied from implicit trust to profound skepticism about the validity of the concordance metric. Survey results suggested a relationship between clinicians' individual differences in learning and failure beliefs, feedback experience, and usability ratings.
Clinicians value feedback on pneumonia diagnoses. Our results highlight the importance of feedback about diagnostic performance and suggest directions for considering individual differences in feedback tool design and implementation.
我们旨在(1)描述急诊科诊断肺炎的过程,(2)研究临床医生对面向临床医生的诊断不一致反馈工具的反应。
我们设计了一种诊断反馈工具,使用电子健康记录数据,根据急诊科临床医生的患者数据,确定 ED 诊断、放射科报告和肺炎出院诊断之间的一致性或不一致性。我们对 11 名急诊科临床医生进行了关于肺炎诊断和对反馈工具反应的半结构式访谈。我们进行了测量思维模式信念、对反馈的舒适度和反馈工具可用性的个体差异的问卷调查。我们对访谈记录进行了定性分析,并对调查数据进行了描述性分析。
主题分析结果显示:(1)ED 中肺炎的诊断过程以诊断不确定性为特征,可能是出于治疗和处理患者的目的;(2)临床医生的诊断自我评估是一个零碎的、不一致的病例回顾和随访过程,反馈工具可以填补这一过程;(3)该反馈工具得到了积极的评价,任务反馈和规范反馈利用了临床医生对高质量患者护理和个人卓越的价值观;(4)对诊断反馈的强烈反应从对一致性指标的有效性的隐含信任到深刻的怀疑不等。调查结果表明,临床医生在学习和失败信念、反馈经验和可用性评分方面存在个体差异。
临床医生重视对肺炎诊断的反馈。我们的结果强调了反馈诊断表现的重要性,并为考虑反馈工具设计和实施中的个体差异提供了方向。