Aguilar-Bretones Muriel, den Hartog Yvette, van Dijk Laura L A, Malahe S Reshwan K, Dieterich Marjolein, Mora Héctor Tejeda, Mueller Yvonne M, Koopmans Marion P G, Reinders Marlies E J, Baan Carla C, van Nierop Gijsbert P, de Vries Rory D
Department of Viroscience, Erasmus Medical Center, Rotterdam, The Netherlands.
Department of Internal Medicine, Nephrology and Transplantation, Erasmus Medical Center Transplant Institute, Rotterdam, The Netherlands.
NPJ Vaccines. 2024 May 28;9(1):93. doi: 10.1038/s41541-024-00886-0.
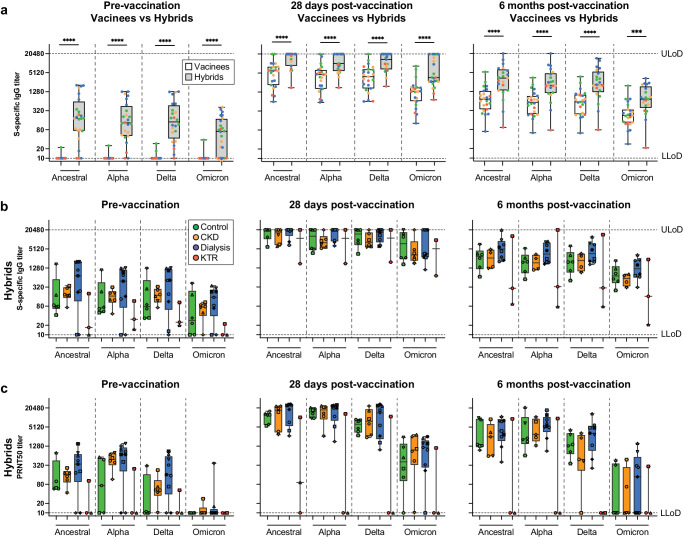
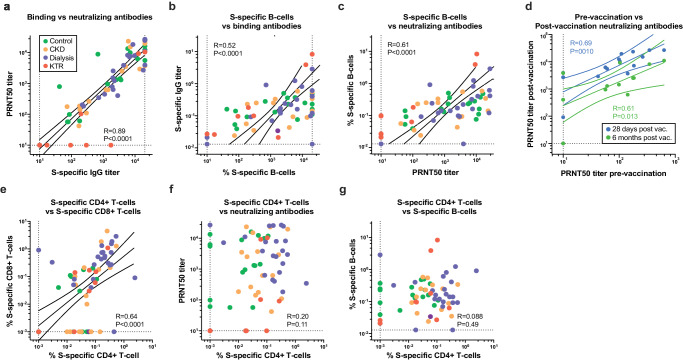
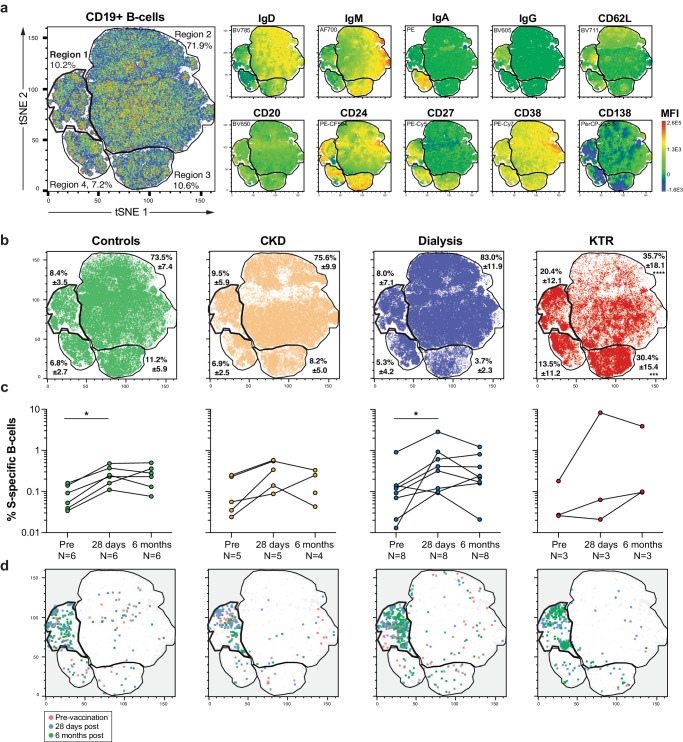
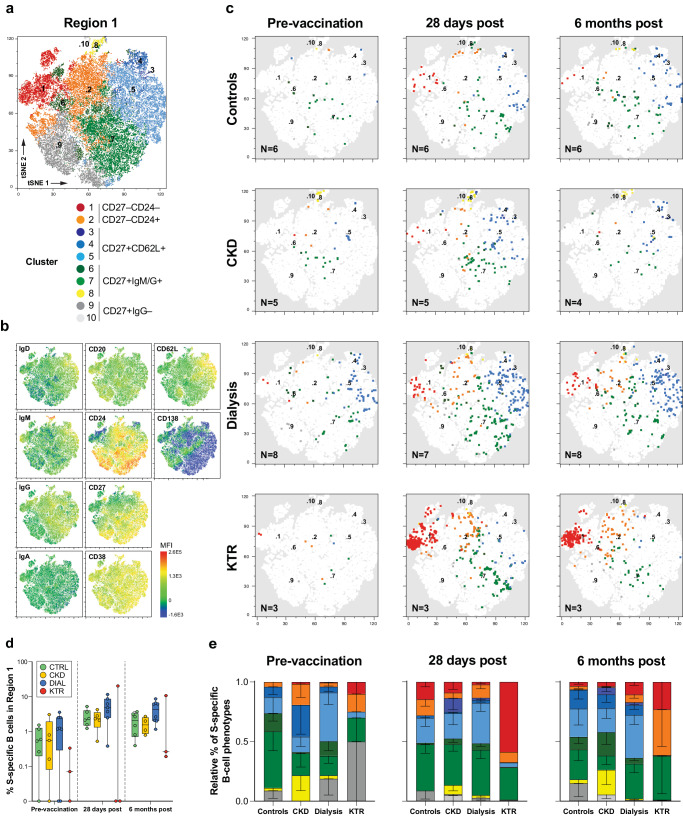
Healthy individuals with hybrid immunity, due to a SARS-CoV-2 infection prior to first vaccination, have stronger immune responses compared to those who were exclusively vaccinated. However, little is known about the characteristics of antibody, B- and T-cell responses in kidney disease patients with hybrid immunity. Here, we explored differences between kidney disease patients and controls with hybrid immunity after asymptomatic or mild coronavirus disease-2019 (COVID-19). We studied the kinetics, magnitude, breadth and phenotype of SARS-CoV-2-specific immune responses against primary mRNA-1273 vaccination in patients with chronic kidney disease or on dialysis, kidney transplant recipients, and controls with hybrid immunity. Although vaccination alone is less immunogenic in kidney disease patients, mRNA-1273 induced a robust immune response in patients with prior SARS-CoV-2 infection. In contrast, kidney disease patients with hybrid immunity develop SARS-CoV-2 antibody, B- and T-cell responses that are equally strong or stronger than controls. Phenotypic analysis showed that Spike (S)-specific B-cells varied between groups in lymph node-homing and memory phenotypes, yet S-specific T-cell responses were phenotypically consistent across groups. The heterogeneity amongst immune responses in hybrid immune kidney patients warrants further studies in larger cohorts to unravel markers of long-term protection that can be used for the design of targeted vaccine regimens.
由于在首次接种疫苗前感染过严重急性呼吸综合征冠状病毒2型(SARS-CoV-2)而具有混合免疫的健康个体,与仅接种疫苗的个体相比,具有更强的免疫反应。然而,对于具有混合免疫的肾病患者的抗体、B细胞和T细胞反应特征知之甚少。在此,我们探讨了无症状或轻度2019冠状病毒病(COVID-19)后具有混合免疫的肾病患者与对照组之间的差异。我们研究了慢性肾病患者、透析患者、肾移植受者以及具有混合免疫的对照组针对初次mRNA-1273疫苗接种的SARS-CoV-2特异性免疫反应的动力学、强度、广度和表型。尽管仅接种疫苗在肾病患者中的免疫原性较低,但mRNA-1273在先前感染过SARS-CoV-2的患者中诱导了强烈的免疫反应。相比之下,具有混合免疫的肾病患者产生的SARS-CoV-2抗体、B细胞和T细胞反应与对照组一样强或更强。表型分析表明,刺突(S)特异性B细胞在淋巴结归巢和记忆表型上在不同组之间存在差异,但S特异性T细胞反应在各表型上在不同组之间是一致的。混合免疫肾病患者免疫反应的异质性需要在更大的队列中进行进一步研究,以揭示可用于设计靶向疫苗方案的长期保护标志物。