Naiditch Hiam, Betts Michael R, Larman H Benjamin, Levi Moshe, Rosenberg Avi Z
Department of Pulmonary, Allergy, Critical Care and Sleep Medicine, University of Pittsburgh, Pittsburgh, PA, United States.
Department of Microbiology and Institute of Immunology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, United States.
Front Immunol. 2025 Feb 12;15:1376654. doi: 10.3389/fimmu.2024.1376654. eCollection 2024.
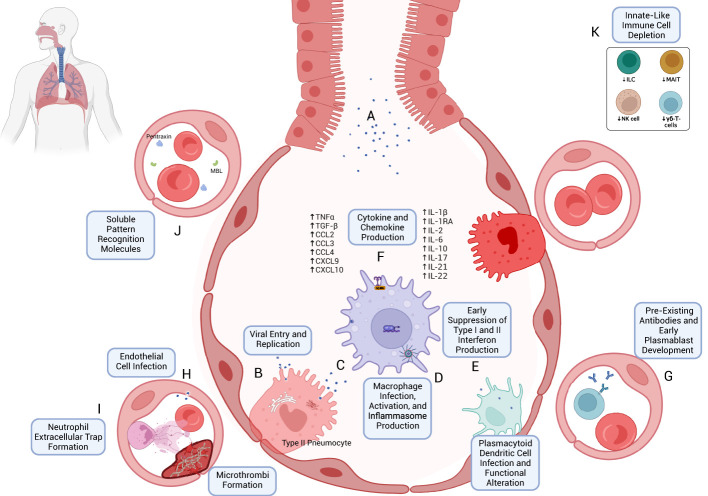
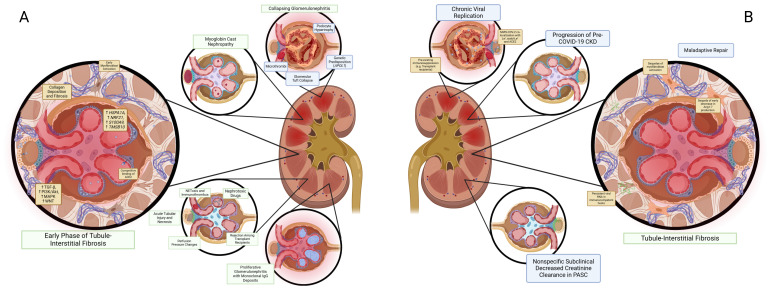
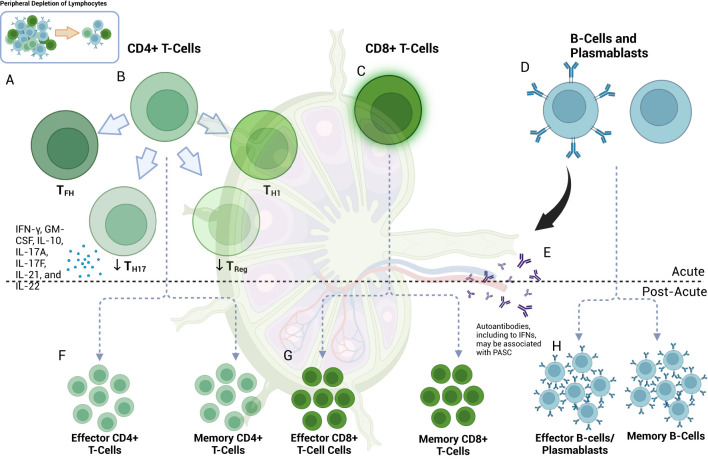
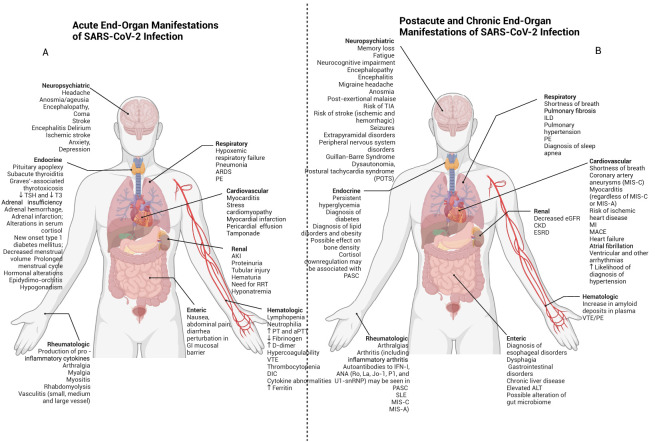
The emergence of the COVID-19 pandemic made it critical to understand the immune and inflammatory responses to the SARS-CoV-2 virus. It became increasingly recognized that the immune response was a key mediator of illness severity and that its mechanisms needed to be better understood. Early infection of both tissue and immune cells, such as macrophages, leading to pyroptosis-mediated inflammasome production in an organ system critical for systemic oxygenation likely plays a central role in the morbidity wrought by SARS-CoV-2. Delayed transcription of Type I and Type III interferons by SARS-CoV-2 may lead to early disinhibition of viral replication. Cytokines such as interleukin-1 (IL-1), IL-6, IL-12, and tumor necrosis factor α (TNFα), some of which may be produced through mechanisms involving nuclear factor kappa B (NF-κB), likely contribute to the hyperinflammatory state in patients with severe COVID-19. Lymphopenia, more apparent among natural killer (NK) cells, CD8+ T-cells, and B-cells, can contribute to disease severity and may reflect direct cytopathic effects of SARS-CoV-2 or end-organ sequestration. Direct infection and immune activation of endothelial cells by SARS-CoV-2 may be a critical mechanism through which end-organ systems are impacted. In this context, endovascular neutrophil extracellular trap (NET) formation and microthrombi development can be seen in the lungs and other critical organs throughout the body, such as the heart, gut, and brain. The kidney may be among the most impacted extrapulmonary organ by SARS-CoV-2 infection owing to a high concentration of ACE2 and exposure to systemic SARS-CoV-2. In the kidney, acute tubular injury, early myofibroblast activation, and collapsing glomerulopathy in select populations likely account for COVID-19-related AKI and CKD development. The development of COVID-19-associated nephropathy (COVAN), in particular, may be mediated through IL-6 and signal transducer and activator of transcription 3 (STAT3) signaling, suggesting a direct connection between the COVID-19-related immune response and the development of chronic disease. Chronic manifestations of COVID-19 also include systemic conditions like Multisystem Inflammatory Syndrome in Children (MIS-C) and Adults (MIS-A) and post-acute sequelae of COVID-19 (PASC), which may reflect a spectrum of clinical presentations of persistent immune dysregulation. The lessons learned and those undergoing continued study likely have broad implications for understanding viral infections' immunologic and inflammatory consequences beyond coronaviruses.
新型冠状病毒肺炎疫情的出现,使得了解对严重急性呼吸综合征冠状病毒2(SARS-CoV-2)病毒的免疫和炎症反应变得至关重要。人们越来越认识到,免疫反应是疾病严重程度的关键调节因素,其机制需要得到更好的理解。组织和免疫细胞(如巨噬细胞)的早期感染,导致在对全身氧合至关重要的器官系统中通过焦亡介导炎性小体产生,这可能在SARS-CoV-2造成的发病机制中起核心作用。SARS-CoV-2对I型和III型干扰素的转录延迟可能导致病毒复制的早期去抑制。白细胞介素-1(IL-1)、IL-6、IL-12和肿瘤坏死因子α(TNFα)等细胞因子,其中一些可能通过涉及核因子κB(NF-κB)的机制产生,可能导致重症新型冠状病毒肺炎患者出现过度炎症状态。淋巴细胞减少在自然杀伤(NK)细胞、CD8+T细胞和B细胞中更为明显,可导致疾病严重程度增加,可能反映了SARS-CoV-2的直接细胞病变效应或终末器官隔离。SARS-CoV-2对内皮细胞的直接感染和免疫激活可能是影响终末器官系统的关键机制。在这种情况下,可在肺部和全身其他关键器官(如心脏、肠道和大脑)中观察到血管内中性粒细胞胞外陷阱(NET)形成和微血栓形成。由于高浓度的血管紧张素转换酶2(ACE2)和暴露于全身性SARS-CoV-2,肾脏可能是受SARS-CoV-2感染影响最严重的肺外器官之一。在肾脏中,急性肾小管损伤、早期肌成纤维细胞激活以及特定人群中的塌陷性肾小球病可能是新型冠状病毒肺炎相关急性肾损伤(AKI)和慢性肾脏病(CKD)发生的原因。特别是新型冠状病毒肺炎相关性肾病(COVAN)的发生可能通过IL-6和信号转导及转录激活因子3(STAT3)信号传导介导,这表明新型冠状病毒肺炎相关免疫反应与慢性疾病的发生之间存在直接联系。新型冠状病毒肺炎的慢性表现还包括儿童多系统炎症综合征(MIS-C)和成人多系统炎症综合征(MIS-A)以及新型冠状病毒肺炎急性后遗症(PASC)等全身性疾病,这可能反映了持续免疫失调的一系列临床表现。所吸取教训以及正在进行的研究可能对理解冠状病毒以外的病毒感染的免疫和炎症后果具有广泛意义。