Jøns Christian, Bloch Thomsen Poul Erik, Riahi Sam, Smilde Tom, Bach Ulrich, Jacobsen Peter Karl, Táborský Miloš, Faluközy Jozsef, Wiemer Marcus, Christensen Per Dahl, Kónyi Attila, Schelfaut Dan, Bulava Alan, Grabowski Marcin, Merkely Béla, Nuyens Dieter, Mahajan Rajiv, Nagel Patrick, Tilz Roland, Malczynski Jerzy, Steinwender Clemens, Brachmann Johannes, Serota Harvey, Schrader Jürgen, Behrens Steffen, Søgaard Peter
Department of Cardiology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark.
Department of Cardiology, Aalborg University Hospital, Aalborg, Denmark.
Front Cardiovasc Med. 2024 May 13;11:1300074. doi: 10.3389/fcvm.2024.1300074. eCollection 2024.
Cardiac arrhythmias predict poor outcome after myocardial infarction (MI). We studied if arrhythmia monitoring with an insertable cardiac monitor (ICM) can improve treatment and outcome.
BIO|GUARD-MI was a randomized, international open-label study with blinded outcome assessment.
Tertiary care facilities monitored the arrhythmias, while the follow-up remained with primary care physicians.
Patients after ST-elevation (STEMI) or non-ST-elevation MI with an ejection fraction >35% and a CHADS-VASc score ≥4 (men) or ≥5 (women).
Patients were randomly assigned to receive or not receive an ICM in addition to standard post-MI treatment. Device-detected arrhythmias triggered immediate guideline recommended therapy changes via remote monitoring.
MACE, defined as a composite of cardiovascular death or acute unscheduled hospitalization for cardiovascular causes.
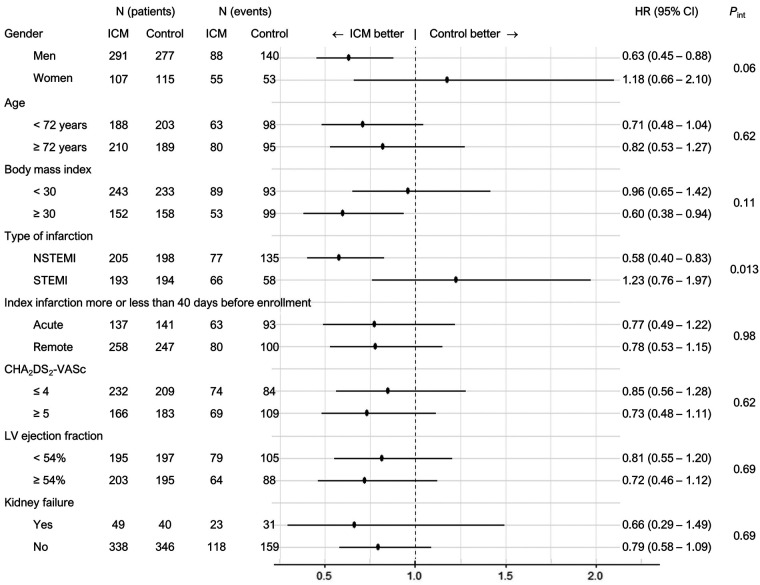
790 patients (mean age 71 years, 72% male, 51% non-STEMI) of planned 1,400 pts were enrolled and followed for a median of 31.6 months. At 2 years, 39.4% of the device group and 6.7% of the control group had their therapy adapted for an arrhythmia [hazard ratio (HR) = 5.9, < 0.0001]. Most frequent arrhythmias were atrial fibrillation, pauses and bradycardia. The use of an ICM did not improve outcome in the entire cohort (HR = 0.84, 95%-CI: 0.65-1.10; = 0.21). In secondary analysis, a statistically significant interaction of the type of infarction suggests a benefit in the pre-specified non-STEMI subgroup. Risk factor analysis indicates that this may be connected to the higher incidence of MACE in patients with non-STEMI.
The burden of asymptomatic but actionable arrhythmias is large in post-infarction patients. However, arrhythmia monitoring with an ICM did not improve outcome in the entire cohort. Post-hoc analysis suggests that it may be beneficial in non-STEMI patients or other high-risk subgroups.
[https://www.clinicaltrials.gov/ct2/show/NCT02341534], NCT02341534.
心律失常预示着心肌梗死(MI)后预后不良。我们研究了使用植入式心脏监测器(ICM)进行心律失常监测是否能改善治疗及预后。
BIO|GUARD-MI是一项随机、国际开放性标签研究,结局评估采用盲法。
三级医疗设施负责监测心律失常,而随访由初级保健医生进行。
ST段抬高型心肌梗死(STEMI)或非ST段抬高型心肌梗死患者,射血分数>35%,CHADS-VASc评分男性≥4或女性≥5。
除标准的心肌梗死后治疗外,患者被随机分配接受或不接受ICM。设备检测到的心律失常通过远程监测触发立即进行指南推荐的治疗调整。
主要不良心血管事件(MACE),定义为心血管死亡或因心血管原因急性非计划住院的综合指标。
计划纳入1400例患者中的790例(平均年龄71岁,72%为男性,51%为非STEMI)入组并随访,中位随访时间为31.6个月。2年时,设备组39.4%的患者和对照组6.7%的患者因心律失常调整了治疗[风险比(HR)=5.9,<0.0001]。最常见的心律失常是心房颤动、停搏和心动过缓。使用ICM并未改善整个队列的预后(HR=0.84, 95%置信区间:0.65-1.10;P=0.21)。在二次分析中,梗死类型的统计学显著交互作用表明在预先指定的非STEMI亚组中有获益。风险因素分析表明这可能与非STEMI患者中较高的MACE发生率有关。
心肌梗死后患者中无症状但可采取行动的心律失常负担很大。然而, 使用ICM进行心律失常监测并未改善整个队列的预后。事后分析表明,它可能对非STEMI患者或其他高危亚组有益处。
[https://www.clinicaltrials.gov/ct2/show/NCT02341534],NCT02341534