Department of Mother and Child, Faculty of Medicine, University of Medicine and Pharmacy "Grigore T. Popa", University Street No. 16, 700115, Iasi, Romania.
Clinical Hospital of Obstetrics and Gynecology "Cuza Voda", Cuza Voda Street No. 34, 700038, Iasi, Romania.
J Assist Reprod Genet. 2024 Jul;41(7):1851-1861. doi: 10.1007/s10815-024-03146-1. Epub 2024 May 29.
To investigate whether the ovarian stimulation with follitropin delta in an individualized algorithm-based manner is inferior to recombinant human-follicle stimulating's follitropin alfa or follitropin beta conventional dosing regarding a series of established primary endpoints.
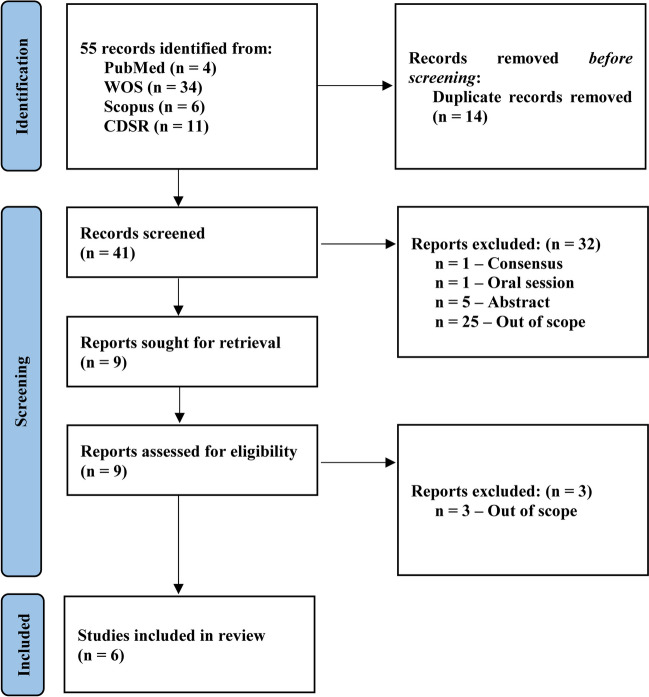
We conducted a registered systematic review (CRD42024512792) on PubMed-MEDLINE, Web of Science™, Cochrane Database of Systematic Reviews, and Scopus. Our search was designed to cover all relevant literature, particularly randomized controlled trials. We critically and comparatively analyzed the outcomes for each primary endpoint based on the intervention, reflected by the positive βhCG test, clinical pregnancy, vital pregnancy, ongoing pregnancy, live birth, live birth at 4 weeks, and multiple pregnancies.
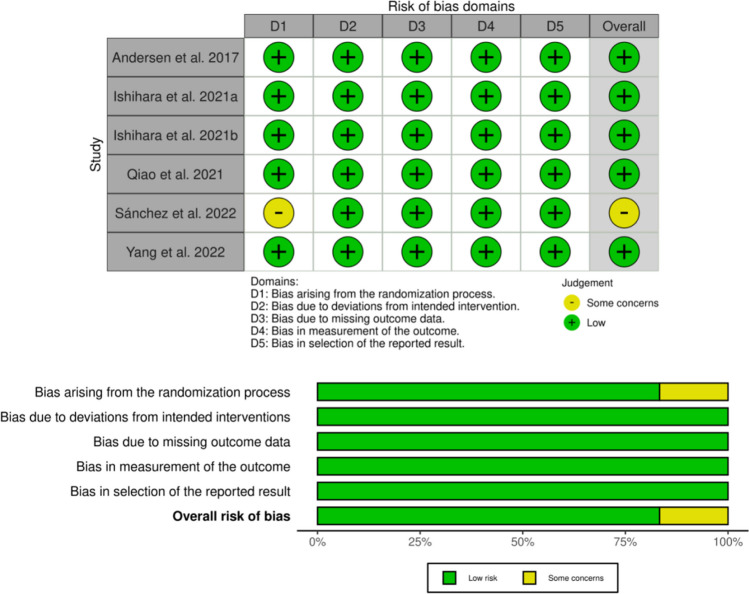
Six randomized controlled trials were included in the quality assessment as priority manuscripts, revealing an 83.3% low risk of bias. Follitropin delta led to non-significant differences in each parameter of interest from positive βhCG test (691; 53.44% vs. 602; 46.55%), ongoing pregnancies (603; 53.79% vs. 518; 46.20%), clinical and vital pregnancies (1,073; 52.80% vs. 959; 47.19%), to live birth and at 4 weeks (595; 54.14% vs. 504; 45.85%) with only 2 losses, and even multiple pregnancies (8; 66.66% vs. 4; 33.33%). However, follitropin delta was well-tolerated among hypo- and hyper-responders without significant risk of ovarian hyperstimulation syndrome and/or preventive interventions in contrast with follitropin alfa or follitropin beta.
The personalized individualized-based algorithm dosing with follitropin delta is non-inferior to conventional follitropin alfa or follitropin beta. It is as effective in promoting a similar response in women without significant comparable adverse effects.
以个体化算法为基础,研究卵泡刺激素 δ 对卵巢的刺激是否不如重组人卵泡刺激素 α 或 β 的常规剂量,针对一系列既定的主要终点。
我们在 PubMed-MEDLINE、Web of Science™、Cochrane 系统评价数据库和 Scopus 上进行了一项已注册的系统评价(CRD42024512792)。我们的搜索旨在涵盖所有相关文献,特别是随机对照试验。我们根据干预措施(阳性βhCG 检测、临床妊娠、活产妊娠、持续妊娠、活产、4 周时活产和多胎妊娠)对每个主要终点的结果进行了批判性和比较性分析。
六项随机对照试验被纳入质量评估作为优先文献,显示出 83.3%的低偏倚风险。卵泡刺激素 δ 在阳性βhCG 检测(691;53.44%对 602;46.55%)、持续妊娠(603;53.79%对 518;46.20%)、临床和活产妊娠(1073;52.80%对 959;47.19%)、活产和 4 周时活产(595;54.14%对 504;45.85%)方面没有显著差异,仅损失 2 例,甚至多胎妊娠(8;66.66%对 4;33.33%)也没有显著差异。然而,与卵泡刺激素 α 或卵泡刺激素 β 相比,卵泡刺激素 δ 在低反应者和高反应者中耐受性良好,没有卵巢过度刺激综合征和/或预防干预的显著风险。
基于个体化的个体化算法剂量的卵泡刺激素 δ 与传统的卵泡刺激素 α 或卵泡刺激素 β 相比不劣效。它在促进女性相似反应方面同样有效,且没有显著的可比不良反应。