Song Yi, Zhou Jianxin, Tan Yun, Wu Yao, Liu Mingdong, Cheng Yuan
Department of Neurosurgery, The Second Affiliated Hospital of Chongqing Medical University, No. 74, Linjiang Road, Yuzhong District, Chongqing, 400010, China.
Department of Neurosurgery, Chongqing University Three Gorges Hospital, No. 165 Xincheng Road, Wanzhou District, Chongqing, 404000, China.
Neurol Ther. 2024 Aug;13(4):1173-1190. doi: 10.1007/s40120-024-00630-9. Epub 2024 May 30.
This study aimed to explore influencing factors and clinical significance of ultra-long-term microischemia following intracranial aneurysm (IA) embolization and establish a theoretical foundation for reducing both the incidence of ultra-long-term microischemia and cognitive dysfunction in patients post embolization.
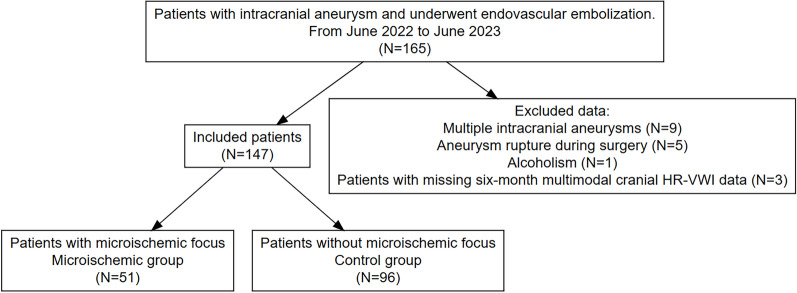
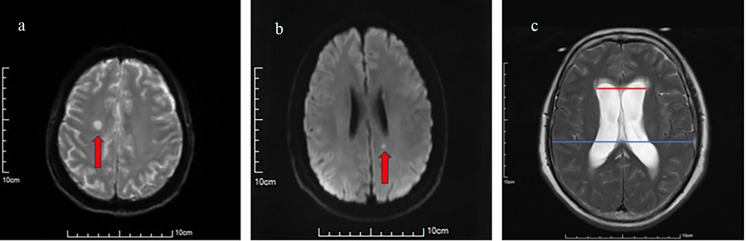
A retrospective analysis was conducted on data from 147 patients who received endovascular treatment for IAs. Patients were categorized into microischemic and control (non-microischemic) groups on the based on the findings of high-resolution magnetic resonance vessel wall imaging (HR-VWI) examinations performed 3 days postoperatively and 6 months postoperatively. Risk factors for the occurrence of ultra-long-term microischemia were determined by univariate analysis and multivariate logistic regression analysis.
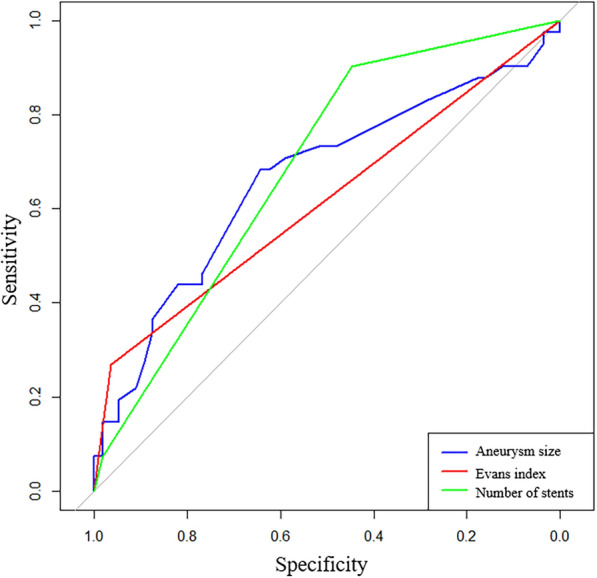
Out of 147 patients included in the study, 51 (34.69%) developed microischemia while the remaining 96 (65.31%) did not experience this condition. Analysis revealed that factors such as sex, age, history of underlying diseases (hypertension, diabetes mellitus), aneurysmal site characteristics, the presence or absence of stenosis in the aneurysm-bearing artery, modified Fisher score at admission, Barthel's index at discharge, immunoinflammatory index at 3 days postoperatively and at the 6-month follow-up, the presence or absence of aneurysmal wall enhancement, and the presence or absence of aneurysmal lumen showed no statistically significant differences between the two groups (all P > 0.05). By contrast, variables like in operative time, rupture status of the aneurysm before surgery according to World Federation of Neurologic Surgeons (WFNS) grade, aneurysm size, number of stents used, number of guidewires and catheters used, and Evans index between the two groups were found to have statistically significant disparities between those who developed microischemia and those who did not (P < 0.05). A subsequent multivariate analysis revealed that aneurysm size, Evans index, and the number of stents used were independent risk factors for the occurrence of ultra-long-term microischemia after surgical intervention of aneurysms (P < 0.05). The receiver operating characteristic (ROC) curves of the patients were constructed on the basis of risk factors determined through multivariate logistic regression analysis. Results indicated that aneurysm size (area under ROC curve (AUC) 0.619, sensitivity 94.7%, specificity 17.1%, P = 0.049), Evans index (AUC 0.670, sensitivity 96.4%, specificity 26.8%, P = 0.004), and number of stents (AUC 0.639, sensitivity 44.6%, specificity 90.2%, P < 0.001) effectively predicted the occurrence of microischemia. The incidence of cognitive dysfunction was higher in the microischemic group than in the control group (P < 0.05), and a greater number of microischemic foci was associated with a higher incidence of cognitive dysfunction. The proportion of microschemia foci in the thalamus and basal ganglia in patients with cognitive dysfunction (60.87%) was significantly higher than that in patients without cognitive dysfunction (34.55%) (P < 0.05).
Aneurysm size, Evans index > 0.3, and the quantity of stents were independent risk factors for the occurrence of ultra-long-term microischemia after aneurysm embolization and provided good predictive performance. Cognitive dysfunction was closely associated with microischemia, with its severity increasing with an increase in the number of ischemic foci.
本研究旨在探讨颅内动脉瘤(IA)栓塞术后超长期微缺血的影响因素及临床意义,为降低栓塞术后患者超长期微缺血及认知功能障碍的发生率奠定理论基础。
对147例行IA血管内治疗的患者的数据进行回顾性分析。根据术后3天和术后6个月进行的高分辨率磁共振血管壁成像(HR-VWI)检查结果,将患者分为微缺血组和对照组(无微缺血组)。通过单因素分析和多因素逻辑回归分析确定超长期微缺血发生的危险因素。
在纳入研究的147例患者中,51例(34.69%)发生微缺血,其余96例(65.31%)未发生该情况。分析显示,性别、年龄、基础疾病史(高血压、糖尿病)、动脉瘤部位特征、载瘤动脉有无狭窄、入院时改良Fisher评分、出院时Barthel指数、术后3天及6个月随访时的免疫炎症指标、动脉瘤壁有无强化以及动脉瘤腔有无等因素在两组间无统计学显著差异(均P>0.05)。相比之下,手术时间、根据世界神经外科联合会(WFNS)分级术前动脉瘤破裂状态、动脉瘤大小、使用支架数量、使用导丝和导管数量以及两组间的Evans指数在发生微缺血者和未发生微缺血者之间存在统计学显著差异(P<0.05)。随后的多因素分析显示,动脉瘤大小、Evans指数和使用支架数量是动脉瘤手术干预后超长期微缺血发生的独立危险因素(P<0.05)。基于多因素逻辑回归分析确定的危险因素构建患者的受试者工作特征(ROC)曲线。结果表明,动脉瘤大小(ROC曲线下面积(AUC)0.619,敏感性94.7%,特异性17.1%,P=0.049)、Evans指数(AUC 0.670,敏感性96.4%,特异性26.8%,P=0.004)和支架数量(AUC 0.639,敏感性44.6%,特异性90.2%,P<0.001)可有效预测微缺血的发生。微缺血组认知功能障碍的发生率高于对照组(P<0.05),且微缺血灶数量越多,认知功能障碍的发生率越高。认知功能障碍患者丘脑和基底节微缺血灶的比例(60.87%)显著高于无认知功能障碍患者(34.55%)(P<0.05)。
动脉瘤大小、Evans指数>0.3以及支架数量是动脉瘤栓塞术后超长期微缺血发生的独立危险因素,且具有良好的预测性能。认知功能障碍与微缺血密切相关,其严重程度随缺血灶数量的增加而加重。