Kurlander Jacob E, Helminski Danielle, Yuan Liyang, Krein Sarah L, Lanham Michael S M, Henstock Jennifer L, Kidwell Kelley M, De Vries Raymond, Resnicow Kenneth, Sholl Haden, Kim Joyce J, Perry Linda K, Parsons Jacqueline, Ha Nghi, Froehlich James B, Aikens James E, Richardson Caroline R, Saini Sameer D, Barnes Geoffrey D
Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, USA.
Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor, Michigan, USA.
Res Pract Thromb Haemost. 2024 Apr 26;8(4):102421. doi: 10.1016/j.rpth.2024.102421. eCollection 2024 May.
Overuse of antiplatelet therapy and underuse of gastroprotection contribute to preventable bleeding in patients taking anticoagulants.
(1) Determine the feasibility of a factorial trial testing patient activation and clinician outreach to reduce gastrointestinal (GI) bleeding risk in patients prescribed warfarin-antiplatelet therapy without proton pump inhibitor gastroprotection and (2) assess intervention acceptability.
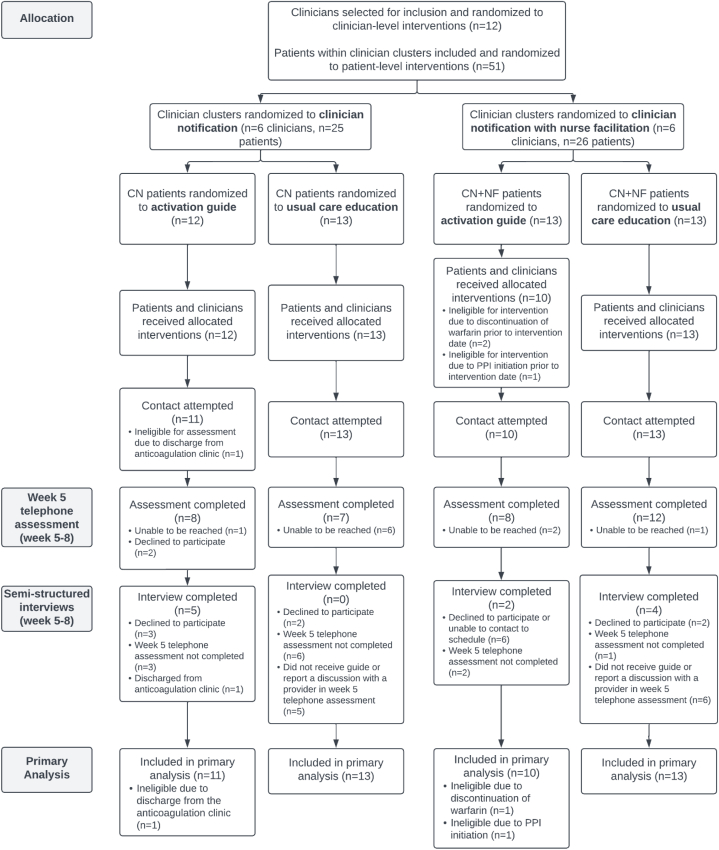
Pragmatic 2 × 2 factorial cluster-randomized controlled pilot comparing (1) a patient activation booklet vs usual care and (2) clinician notification vs clinician notification plus nurse facilitation was performed. The primary feasibility outcome was percentage of patients completing a structured telephone assessment after 5 weeks. Exploratory outcomes, including effectiveness, were evaluated using chart review, surveys, and semistructured interviews.
Among 47 eligible patients, 35/47 (74.5%; 95% CI, 58.6%-85.7%) met the feasibility outcome. In the subset confirmed to be high risk for upper GI bleeding, 11/29 (37.9%; 95% CI, 16.9%-64.7%) made a medication change, without differences between intervention arms. In interviews, few patients reported reviewing the activation booklet; barriers included underestimating GI bleeding risk, misunderstanding the booklet's purpose, and receiving excessive health communication materials. Clinicians responded to notification messages for 24/47 patients (51.1%; 95% CI, 26.4%-75.4%), which was lower for surgeons than nonsurgeons (22.7% vs 76.0%). Medical specialists but not surgeons viewed clinician notification as acceptable.
The proposed trial design and outcome ascertainment strategy were feasible, but the patient activation intervention is unlikely to be effective as designed. While clinician notification appears promising, it may not be acceptable to surgeons, findings which support further refinement and testing of a clinician notification intervention.
抗血小板治疗的过度使用和胃保护措施的不足导致服用抗凝剂的患者出现可预防的出血。
(1)确定一项析因试验的可行性,该试验测试患者激活和临床医生外展服务,以降低接受华法林-抗血小板治疗且未使用质子泵抑制剂进行胃保护的患者的胃肠道(GI)出血风险,以及(2)评估干预措施的可接受性。
进行了一项实用的2×2析因整群随机对照试验,比较(1)患者激活手册与常规护理,以及(2)临床医生通知与临床医生通知加护士协助。主要可行性结局是5周后完成结构化电话评估的患者百分比。使用病历审查、调查和半结构化访谈评估包括有效性在内的探索性结局。
在47名符合条件的患者中,35/47(74.5%;95%CI,58.6%-85.7%)达到了可行性结局。在被确认为上消化道出血高风险的亚组中,11/29(37.9%;95%CI,16.9%-64.7%)进行了药物调整,各干预组之间无差异。在访谈中,很少有患者报告阅读了激活手册;障碍包括低估胃肠道出血风险、误解手册目的以及收到过多的健康宣传材料。临床医生对47名患者中的24名(51.1%;95%CI,26.4%-75.4%)回复了通知信息,外科医生的回复率低于非外科医生(22.7%对76.0%)。医学专家而非外科医生认为临床医生通知是可接受的。
拟议的试验设计和结局确定策略是可行的,但患者激活干预按设计不太可能有效。虽然临床医生通知似乎有前景,但外科医生可能无法接受,这些发现支持对临床医生通知干预进行进一步完善和测试。