Griffith Averil, Golden Alyssa R, Lefebvre Brigitte, McGeer Allison, Tyrrell Gregory J, Zhanel George G, Kus Julianne V, Hoang Linda, Minion Jessica, Van Caeseele Paul, Smadi Hanan, Haldane David, Yu Yang, Ding Xiaofeng, Steven Laura, McFadzen Jan, Franklin Kristyn, Martin Irene
National Microbiology Laboratory, Public Health Agency of Canada, Winnipeg, MB.
Laboratoire de santé publique du Québec, Sainte-Anne-de- Bellevue, QC.
Can Commun Dis Rep. 2024 May 24;50(5):121-134. doi: 10.14745/ccdr.v50i05a02.
Invasive pneumococcal disease (IPD, ) has been a nationally notifiable disease in Canada since 2000. The use of conjugate vaccines has caused a shift in the distribution of serotypes over time. This report is a summary of the demographics, serotypes and antimicrobial resistance of IPD isolates collected in Canada in 2021 and 2022.
The National Microbiology Laboratory (NML) of the Public Health Agency of Canada in Winnipeg, Manitoba collaborates with provincial and territorial public health laboratories to conduct national surveillance of IPD. There were 1,999 isolates reported in 2021 and 3,775 isolates in 2022. Serotype was determined by the Quellung reaction or whole-genome sequencing (WGS). Antimicrobial susceptibilities were determined by WGS methods, broth microdilution, or data shared by collaborators in the Canadian Antimicrobial Resistance Alliance program at the University of Manitoba. Population-based IPD incidence rates were obtained through the Canadian Notifiable Disease Surveillance System.
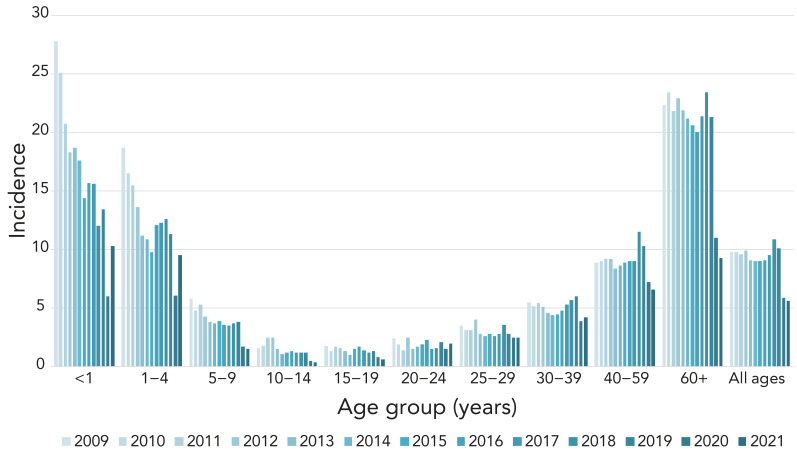
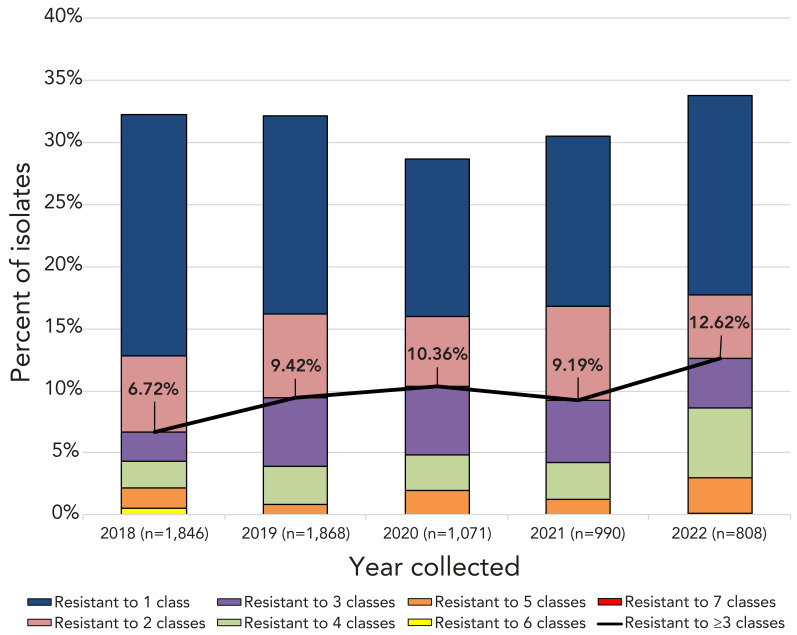
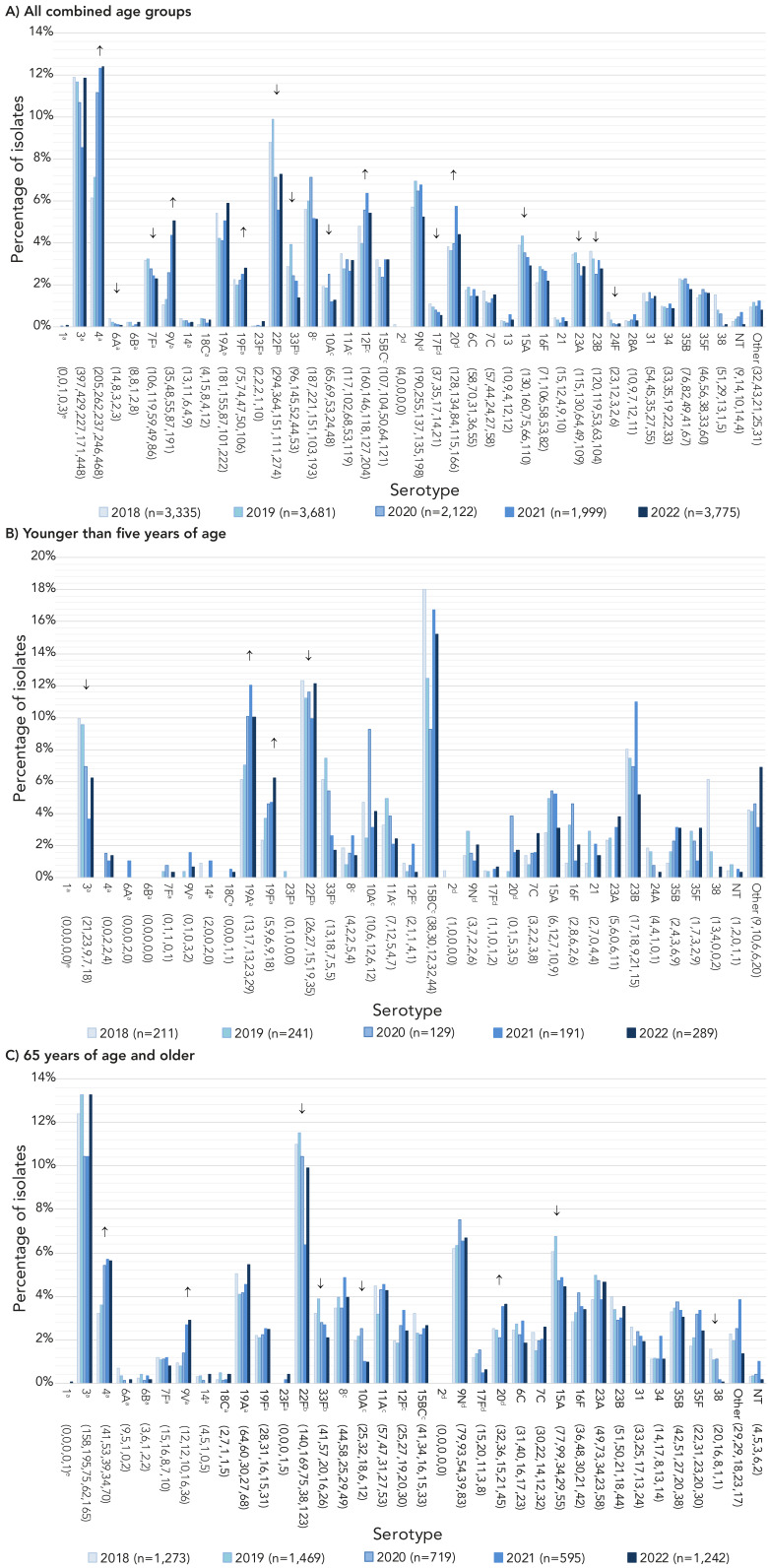
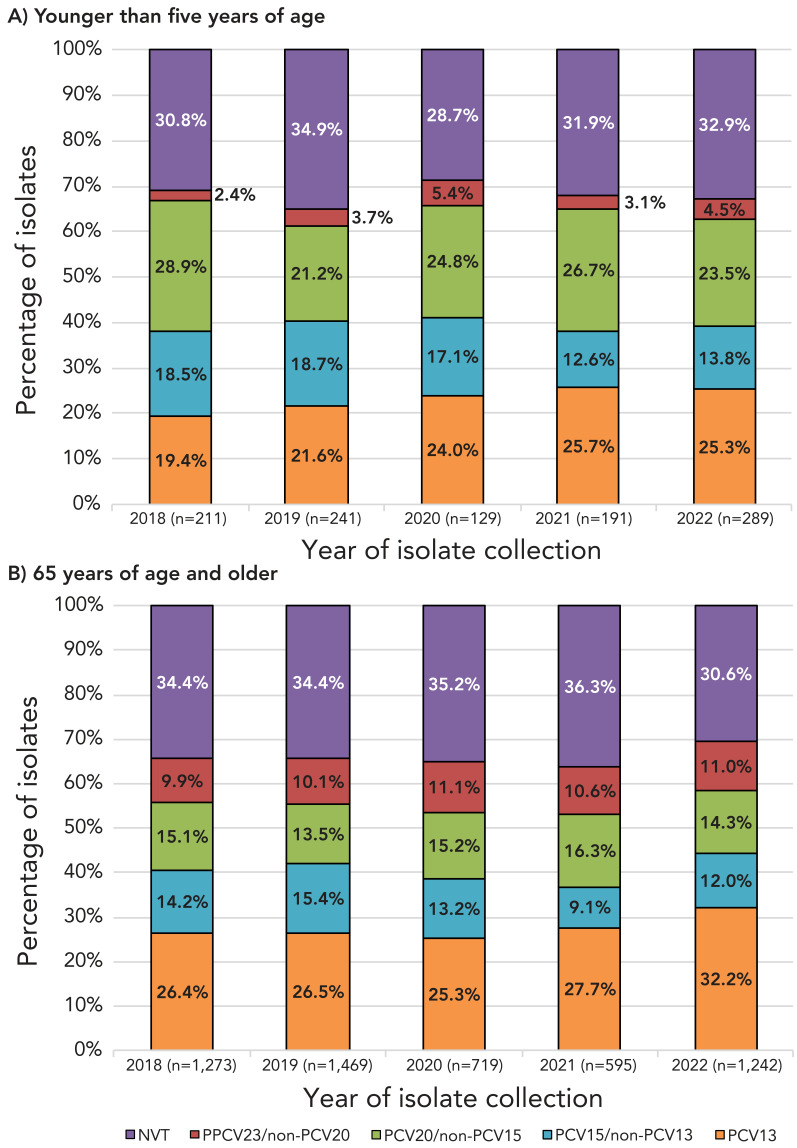
The incidence of IPD in Canada was 5.62 cases per 100,000 population in 2021, decreasing from the peak of 10.86 cases per 100,000 population in 2018. Serotypes with increasing trends (<0.05) between 2018 and 2022 included: 4 (6.1%-12.4%), 9V (1.0%-5.1%) and 12F (4.8%-5.4%). The overall prevalence of PCV13 serotypes increased over the same period (31.2%-41.5%, <0.05) while the prevalence of non-vaccine types decreased significantly (27.3%-21.5%, <0.0001). The highest rates of antimicrobial resistance in 2021 and 2022 were seen with clarithromycin (21%, 2021; 24%, 2022) and erythromycin (22%, 2021; 24%, 2022). Multidrug-resistant IPD continued to increase from 2018 to 2022 (6.7%-12.6%, <0.05).
The number of cases of IPD continued to decrease in 2021 in comparison to previous years, however, 2022 saw a return to pre-COVID-19 levels. Disease due to PCV13 serotypes 3, 4, 9V and 19F, as well as non-PCV13 serotypes 12F and 20, is increasing in prevalence. Surveillance of IPD to monitor changing serotype distribution and antimicrobial resistance is essential.
自2000年以来,侵袭性肺炎球菌疾病(IPD)在加拿大属于国家法定报告疾病。随着时间的推移,结合疫苗的使用导致了血清型分布的变化。本报告总结了2021年和2022年在加拿大收集的IPD分离株的人口统计学特征、血清型和抗菌药物耐药性。
位于曼尼托巴省温尼伯市的加拿大公共卫生署国家微生物实验室(NML)与各省和地区的公共卫生实验室合作,对IPD进行全国监测。2021年报告了1999株分离株,2022年报告了3775株分离株。血清型通过荚膜肿胀反应或全基因组测序(WGS)确定。抗菌药物敏感性通过WGS方法、肉汤微量稀释法或曼尼托巴大学加拿大抗菌药物耐药性联盟项目中的合作者共享的数据确定。基于人群的IPD发病率通过加拿大法定疾病监测系统获得。
2021年加拿大IPD的发病率为每10万人5.62例,低于2018年每10万人10.86例的峰值。2018年至2022年期间呈上升趋势(<0.05)的血清型包括:4型(6.1%-12.4%)、9V型(1.0%-5.1%)和12F型(4.8%-5.4%)。同期,PCV13血清型的总体流行率有所上升(31.2%-41.5%,<0.05),而非疫苗型的流行率显著下降(27.3%-21.5%,<0.0001)。2021年和2022年,对克拉霉素的耐药率最高(2021年为21%;2022年为24%),对红霉素的耐药率次之(2021年为22%;2022年为24%)。2018年至2022年,多重耐药IPD持续增加(6.7%-12.6%,<0.05)。
与前几年相比,2021年IPD病例数持续下降,但2022年又恢复到了新冠疫情前的水平。由PCV13血清型3、4、9V和19F以及非PCV13血清型12F和20引起的疾病流行率正在上升。监测IPD以监测血清型分布和抗菌药物耐药性的变化至关重要。