Redondo Ana, Austin Conal
Congenital Cardiac Surgery Department, Evelina London Children's Hospital, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom.
JTCVS Tech. 2024 Feb 14;24:121-127. doi: 10.1016/j.xjtc.2024.02.004. eCollection 2024 Apr.
The Ross operation is a widely accepted option for aortic valve replacement in children, and evidence shows its excellent results in terms of hemodynamics and durability. However, indications are still limited due to the fact that it is a technically demanding procedure, only performed by specialized surgeons. On top of that, and despite numerous techniques being applied, autograft dilatation remains a key disadvantage, which can lead to graft failure. In recent years, the ExoVasc Personalized External Aortic Root Support (PEARS) has proven to be a safe and effective option to prevent aortic root dilatation in various aortopathies and is a technique that lends itself to support the pulmonary autograft in the Ross operation.
During the past 7 years, we have used the ExoVasc PEARS graft, manufactured from the patients' pulmonary artery measurements from computed tomography scan data, to support the pulmonary autograft in the Ross operation. This graft (manufactured by Exstent Ltd, UK) is implanted at the same time as the autograft. We have reviewed all the patients who underwent this surgery, including demographic data, aorta measurements, operative data, and follow-up assessment consisting of periodic echocardiograms and magnetic resonance imaging scans.
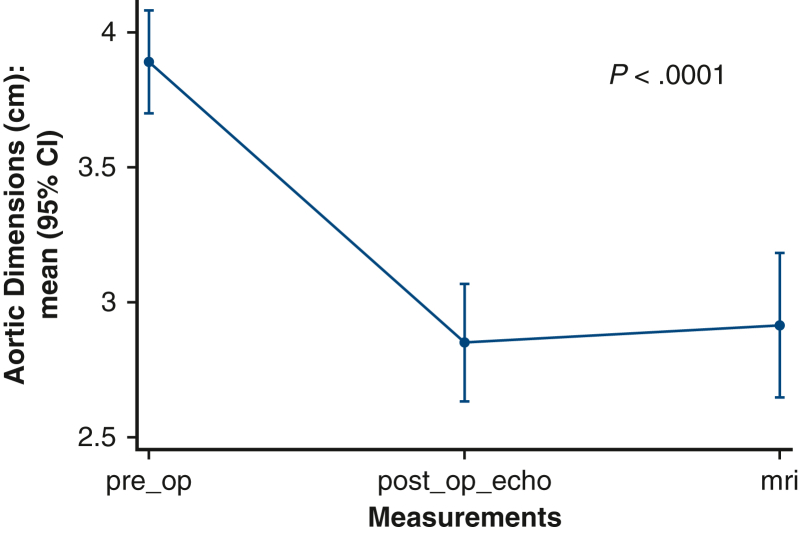
Fifty patients were included in the study. Mean age at the time of the operation was 29.84 years, the youngest patient was 9 years-old. Nineteen patients (38%) had previous sternotomies; 11 of them having had a previous aortic valve replacement. Seventy-two percent of patients had initially a bicuspid aortic valve. Mean diameter of the ascending aorta was 3.83 cm. Forty-four percent of patients required a concomitant reduction aortoplasty due to mismatch sizes between the ascending aorta and the autograft. Mean bypass and crossclamp times were 200.66 and 151.14 minutes, respectively. Median length of stay was 6 days. Mean follow-up was 16.88 months. Two patients required subsequent aortic valve replacement (1 had rheumatic valve disease and the other had iatrogenic damage in his autograft valve leaflet). Ascending aorta dimensions remain stable when compared with immediate postoperative studies. There were no deaths.
The ExoVasc PEARS graft has proven to be an excellent support in the Ross operation to prevent the autograft failure related to autograft dilatation that can offer several advantages compared with other existing techniques. With this type of support, we believe the Ross indications can be expanded to multiple clinical scenarios, given the good long-term results this operation offers in terms of durability, life expectancy, and hemodynamics.
罗斯手术是儿童主动脉瓣置换术广泛接受的一种选择,有证据表明其在血流动力学和耐用性方面效果极佳。然而,由于该手术技术要求高,仅由专业外科医生实施,其适应症仍然有限。除此之外,尽管应用了多种技术,但自体移植物扩张仍是一个关键缺点,可能导致移植物失败。近年来,ExoVasc个性化体外主动脉根部支撑装置(PEARS)已被证明是预防各种主动脉病变中主动脉根部扩张的一种安全有效的选择,并且是一种有助于在罗斯手术中支撑肺动脉自体移植物的技术。
在过去7年中,我们使用根据计算机断层扫描数据测量的患者肺动脉制造的ExoVasc PEARS移植物,在罗斯手术中支撑肺动脉自体移植物。该移植物(由英国Exstent有限公司制造)与自体移植物同时植入。我们回顾了所有接受该手术的患者,包括人口统计学数据、主动脉测量值、手术数据以及由定期超声心动图和磁共振成像扫描组成的随访评估。
50例患者纳入研究。手术时的平均年龄为29.84岁,最年轻的患者为9岁。19例患者(38%)曾接受过胸骨切开术;其中11例曾接受过主动脉瓣置换术。72%的患者最初为二叶式主动脉瓣。升主动脉平均直径为3.83厘米。44%的患者因升主动脉与自体移植物尺寸不匹配需要同时进行升主动脉缩窄成形术。平均体外循环和主动脉阻断时间分别为200.66分钟和151.14分钟。中位住院时间为6天。平均随访时间为16.88个月。2例患者随后需要进行主动脉瓣置换术(1例患有风湿性瓣膜病,另1例自体移植物瓣膜小叶有医源性损伤)。与术后即刻检查相比,升主动脉尺寸保持稳定。无死亡病例。
ExoVasc PEARS移植物已被证明在罗斯手术中是一种极好的支撑物,可预防与自体移植物扩张相关的自体移植物失败,与其他现有技术相比具有多个优点。有了这种支撑,鉴于该手术在耐用性、预期寿命和血流动力学方面的良好长期效果,我们认为罗斯手术的适应症可以扩大到多种临床情况。