Nørregaard Jakobsen Frederikke, Sandgaard Niels Christian Foldager, Olsen Thomas, Brandes Axel, Djurhuus Mogens Stig, Schæffer Mie, Mejldal Anna, Jørgensen Ole Dan, Johansen Jens Brock
Department of Cardiology, Odense University Hospital, Odense, Denmark.
Open Patient Data Explorative Network, Odense University Hospital, Odense, Denmark.
Heart Rhythm O2. 2024 Apr 5;5(5):281-288. doi: 10.1016/j.hroo.2024.04.001. eCollection 2024 May.
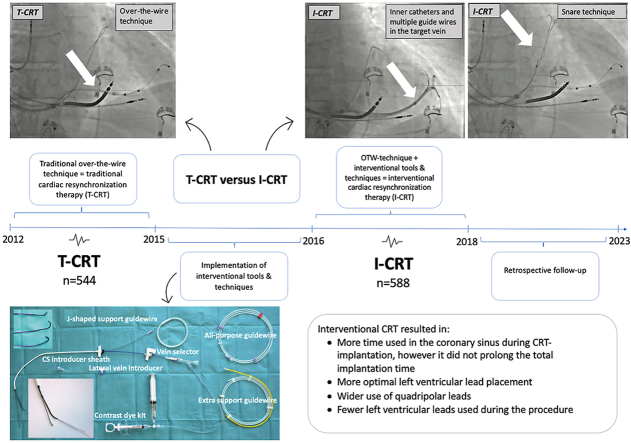
Interventional cardiac resynchronization therapy (I-CRT) for left ventricular lead (LVL) placement works as a supplement to traditional (over-the-wire) cardiac resynchronization therapy (T-CRT). It has been argued that I-CRT is a time-consuming and complicated procedure.
The purpose of this study was to investigate differences in procedure-related, perioperative, postoperative, and clinical endpoints between I-CRT and T-CRT.
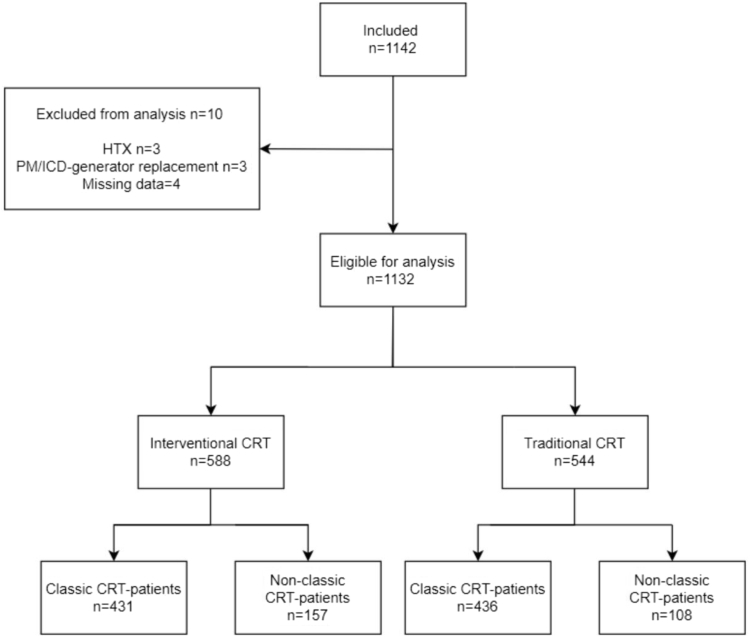
This single-center, retrospective, cohort study included all consecutive patients receiving a CRT-pacemaker/defibrillator between January 1, 2012, and August 31, 2018. Patients underwent T-CRT from January 1, 2012, to June 1, 2015, and I-CRT from January 1, 2016, to August 31, 2018. We obtained data from patient record files, fluoroscopic images, and the Danish Pacemaker and ICD Register. Data were analyzed using Wilcoxon rank-sum/linear regression for continuous variables and the Pearson χ/Fisher exact for categorical variables.
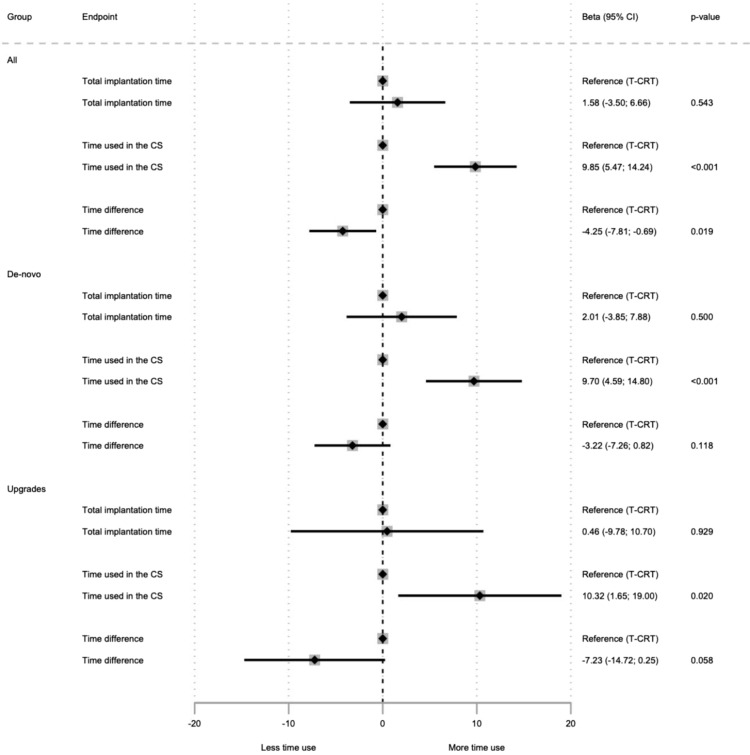
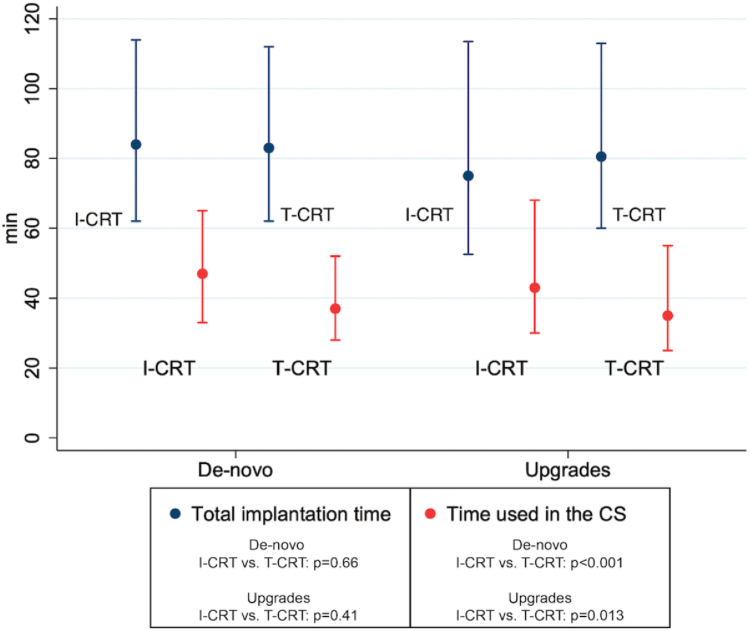
Optimal LVL placement was achieved in 82.7% of the I-CRT group and 76.8% of the T-CRT group ( = .015). In the I-CRT group, 99.0% of LVLs were quadripolar vs 55.3% in the T-CRT group ( <.001). Two or more leads were used during the procedure in 0.7% and 10.5% of all cases in the I-CRT and T-CRT groups, respectively ( <.001). Total implantation time was 81.0 minutes in the I-CRT group and 83.0 minutes in the T-CRT group ( = .41). Time with catheters in the coronary sinus was 45.0 minutes for the I-CRT group vs 37.0 minutes in the T-CRT group, respectively ( <.001).
I-CRT did not prolong total implantation time despite longer time with catheters in the coronary sinus. I-CRT allowed more optimal LVL placement, wider use of quadripolar leads, and use of fewer leads during the procedure.
用于左心室导线(LVL)植入的介入性心脏再同步治疗(I-CRT)是传统(经钢丝)心脏再同步治疗(T-CRT)的一种补充。有人认为I-CRT是一个耗时且复杂的过程。
本研究的目的是调查I-CRT和T-CRT在手术相关、围手术期、术后及临床终点方面的差异。
这项单中心、回顾性队列研究纳入了2012年1月1日至2018年8月31日期间所有连续接受CRT起搏器/除颤器的患者。患者在2012年1月1日至2015年6月1日期间接受T-CRT,在2016年1月1日至2018年8月31日期间接受I-CRT。我们从患者病历档案、荧光透视图像以及丹麦起搏器和植入式心律转复除颤器登记处获取数据。对于连续变量,使用Wilcoxon秩和/线性回归进行数据分析;对于分类变量,使用Pearson χ²检验/Fisher精确检验进行数据分析。
I-CRT组82.7%的患者实现了最佳LVL植入,T-CRT组为76.8%(P = 0.015)。I-CRT组99.0%的LVL为四极导线,而T-CRT组为55.3%(P < 0.001)。I-CRT组和T-CRT组分别有0.7%和10.5%的所有病例在手术过程中使用了两根或更多导线(P < 0.001)。I-CRT组的总植入时间为81.0分钟,T-CRT组为83.0分钟(P = 0.41)。I-CRT组冠状动脉窦内导管留置时间为45.0分钟,T-CRT组为37.0分钟(P < 0.001)。
尽管I-CRT组冠状动脉窦内导管留置时间更长,但并未延长总植入时间。I-CRT能实现更优化的LVL植入,更广泛地使用四极导线,且手术过程中使用的导线数量更少。