Division of Nephrology, Department of Medicine, Virginia Commonwealth University, Richmond, VA.
Department of Biostatistics, Virginia Commonwealth University, Richmond, VA.
PLoS One. 2024 Jun 6;19(6):e0301425. doi: 10.1371/journal.pone.0301425. eCollection 2024.
The influence of center volume on kidney transplant outcomes is a topic of ongoing debate. In this study, we employed competing risk analyses to accurately estimate the marginal probability of graft failure in the presence of competing events, such as mortality from other causes with long-term outcomes. The incorporation of immunosuppression protocols and extended follow-up offers additional insights. Our emphasis on long-term follow-up aligns with biological considerations where competing risks play a significant role.
We examined data from 219,878 adult kidney-only transplantations across 256 U.S. transplant centers (January 2001-December 2015) sourced from the Organ Procurement and Transplantation Network registry. Centers were classified into quartiles by annual volume: low (Q1 = 28), medium (Q2 = 75), medium-high (Q3 = 121), and high (Q4 = 195). Our study investigated the relationship between center volume and 5-year outcomes, focusing on graft failure and mortality. Sub-population analyses included deceased donors, living donors, diabetic recipients, those with kidney donor profile index >85%, and re-transplants from deceased donors.
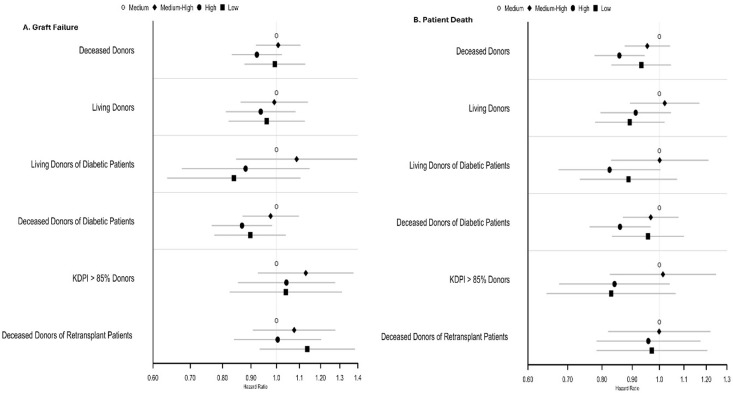
Adjusted cause-specific hazard ratios (aCHR) for Five-Year Graft Failure and Patient Death were examined by center volume, with low-volume centers as the reference standard (aCHR: 1.0). In deceased donors, medium-high and high-volume centers showed significantly lower cause-specific hazard ratios for graft failure (medium-high aCHR = 0.892, p<0.001; high aCHR = 0.953, p = 0.149) and patient death (medium-high aCHR = 0.828, p<0.001; high aCHR = 0.898, p = 0.003). Among living donors, no significant differences were found for graft failure, while a trend towards lower cause-specific hazard ratios for patient death was observed in medium-high (aCHR = 0.895, p = 0.107) and high-volume centers (aCHR = 0.88, p = 0.061).
Higher center volume is associated with significantly lower cause-specific hazard ratios for graft failure and patient death in deceased donors, while a trend towards reduced cause-specific hazard ratios for patient death is observed in living donors.
中心容量对肾移植结果的影响是一个持续争论的话题。在这项研究中,我们采用竞争风险分析来准确估计在存在竞争事件(如其他原因导致的死亡率和长期结果)的情况下移植物失败的边缘概率。纳入免疫抑制方案和延长随访时间提供了额外的见解。我们强调长期随访与生物学考虑因素一致,其中竞争风险起着重要作用。
我们检查了 256 个美国移植中心(2001 年 1 月至 2015 年 12 月)的 219878 例成人肾移植的数据,这些数据来源于器官采购与移植网络登记处。中心按年度容量分为四组:低容量(Q1 = 28)、中容量(Q2 = 75)、中高容量(Q3 = 121)和高容量(Q4 = 195)。我们的研究调查了中心容量与 5 年结果之间的关系,重点是移植物失败和死亡率。子人群分析包括已故供体、活体供体、糖尿病受者、肾供体指数>85%的受者以及来自已故供体的再移植受者。
按中心容量调整了 5 年移植物失败和患者死亡的特定原因危险比(aCHR),低容量中心作为参考标准(aCHR:1.0)。在已故供体中,中高和高容量中心的移植物失败特定原因危险比显著降低(中高 aCHR = 0.892,p<0.001;高 aCHR = 0.953,p = 0.149)和患者死亡(中高 aCHR = 0.828,p<0.001;高 aCHR = 0.898,p = 0.003)。在活体供体中,移植物失败没有发现显著差异,而中高(aCHR = 0.895,p = 0.107)和高容量中心(aCHR = 0.88,p = 0.061)患者死亡的特定原因危险比呈下降趋势。
在已故供体中,中心容量较高与移植物失败和患者死亡的特定原因危险比显著降低相关,而在活体供体中,患者死亡的特定原因危险比呈下降趋势。