Department of Hand Surgery, Shanghai General Hospital, Shanghai Jiao Tong University, School of Medicine, 650 New Songjiang Road, Songjiang, Shanghai, 201620, China.
Department of Hand Surgery, Affiliated Hospital of Nantong University, 20 West Temple Road, Nantong, Jiangsu, 226001, China.
BMC Musculoskelet Disord. 2024 Jun 6;25(1):448. doi: 10.1186/s12891-024-07561-4.
Fractures of the scaphoid are the most common carpal injuries, account for 80-90% of all carpal fractures. 5-15% nonunion of scaphoid fractures were reported even with adequate primary treatment, which probably progresses to osteoarthritic changes several decades later. Researches regarding to scaphoid physiological characteristic in vitro and in vivo and kinds of trials in clinical practice are being kept on going, which contribute much to our clinical practice. With the advancing wrist arthroscopy, 3D-print patient-specific drill guide, and intraoperative fluoroscopic guidance, dorsal approach (mini-invasive and percutaneous technique) is being popular, through which we can implant the screw in good coincidence with biomechanics and with less disturbing tenuous blood supply of the scaphoid. Investigating the noncontact area of the dorsal proximal scaphoid in different wrist positions can facilitate preoperatively estimating insert point of the screw.
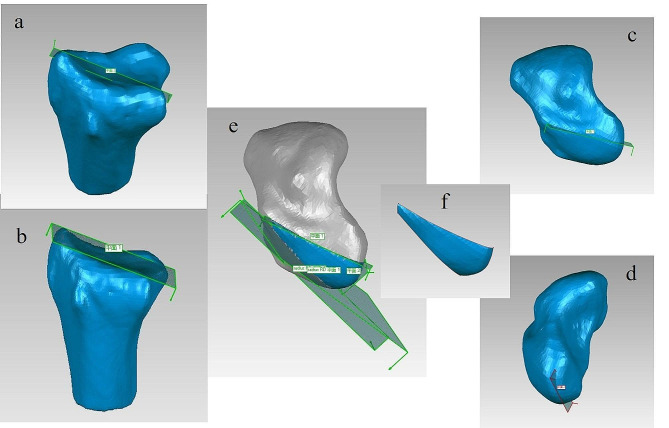
Eight volunteers were recruited to accept CT scans in six extreme wrist positions. The images of DICOM mode were imput into the Mimics analytical system, the segmented scaphoid, lunate and radius were exported in mode of ASCII STL and were opened in the software of Geomagic studio. We created four planes based on anatomic markers on the surface of the radius and scaphoid to confine the proximal scaphoid to form the so-called non-contact regions. We measured and compared the areas in six targeted positions.
Amidst six extreme wrist positions, area of the non-contact region in extreme dorsal extension (59.81 ± 26.46 mm) was significantly the smallest, and it in extreme palmar flexion significantly was largest (170.51 ± 30.44 mm). The non-contact regions increased in order of dorsal extension, supination, ulnar deviation, radial deviation, pronation and palmar flexion. As for two-group comparison, the non-contact region showed significantly larger (p < 0.05) in palmar flexion than the others except for in pronation individually, and in radial deviation (p < 0.05) than in dorsal extension.
Sufficient space was available for the screw started from the dorsal approach despite the wrist positions.
舟状骨骨折是最常见的腕骨损伤,占所有腕骨骨折的 80-90%。即使采用适当的初次治疗,仍有 5-15%的舟状骨骨折不愈合,可能在几十年后发展为骨关节炎改变。关于舟状骨在体外和体内的生理特性以及临床实践中的各种试验的研究一直在进行,这对我们的临床实践有很大的帮助。随着腕关节镜技术的进步,3D 打印患者特异性钻头导向器和术中透视引导的出现,背侧入路(微创和经皮技术)越来越受欢迎,通过这种方法,我们可以将螺钉植入到与生物力学相吻合的位置,并且对舟状骨脆弱的血供干扰较小。研究不同腕关节位置时背侧近侧舟状骨的非接触区,可以帮助术前估计螺钉的插入点。
招募了 8 名志愿者进行 6 种极端腕关节位置的 CT 扫描。DICOM 模式的图像被输入 Mimics 分析系统,以 ASCII STL 模式导出分割的舟状骨、月骨和桡骨,并在 Geomagic Studio 软件中打开。我们基于桡骨和舟状骨表面的解剖标记创建了四个平面,以限制近侧舟状骨形成所谓的非接触区。我们测量并比较了 6 个目标位置的面积。
在 6 种极端腕关节位置中,极度背伸位(59.81±26.46mm)的非接触区最小,极度掌屈位(170.51±30.44mm)最大。非接触区依次为背伸、旋前、尺偏、桡偏、旋前和掌屈增加。对于两组比较,除了单独的旋前位外,掌屈位的非接触区明显大于其他位置(p<0.05),桡偏位的非接触区也明显大于背伸位(p<0.05)。
尽管腕关节位置不同,但从背侧入路开始,螺钉仍有足够的空间。