Department of Radiology, University Hospital, LMU Munich, Marchioninistr. 15, 81377, Munich, Germany.
Department of Medicine III, University Hospital, LMU Munich, Munich, Germany.
Cancer Imaging. 2024 Jun 7;24(1):70. doi: 10.1186/s40644-024-00708-5.
To assess the eligibility of patients with advanced or recurrent solid malignancies presented to a molecular tumor board (MTB) at a large precision oncology center for inclusion in trials with the endpoints objective response rate (ORR) or duration of response (DOR) based on Response Evaluation Criteria in Solid Tumors (RECIST version 1.1).
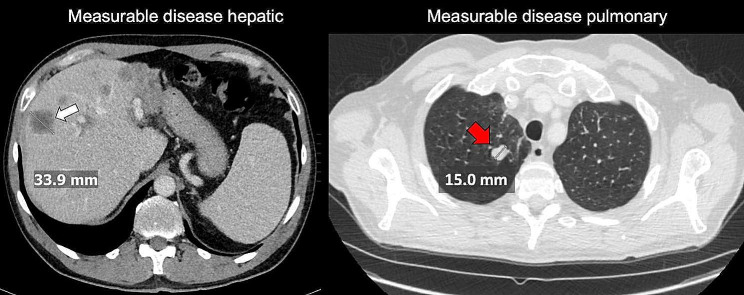
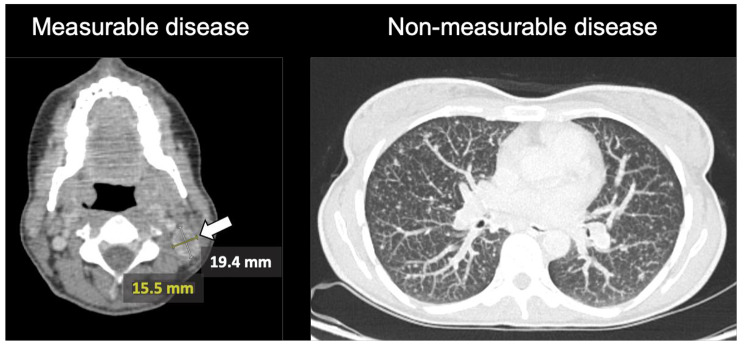
Prospective patients with available imaging at the time of presentation in the MTB were included. Imaging data was reviewed for objectifiable measurable disease (MD) according to RECIST v1.1. Additionally, we evaluated the patients with MD for representativeness of the identified measurable lesion(s) in relation to the overall tumor burden.
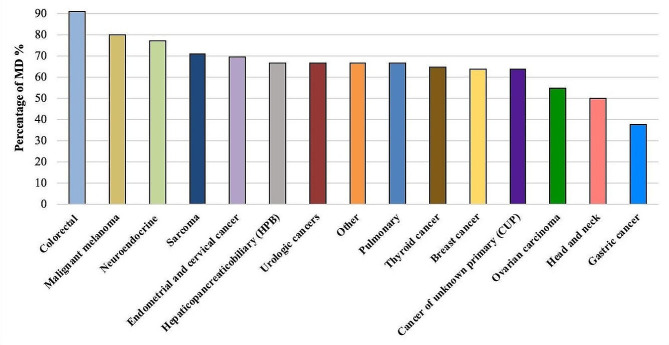
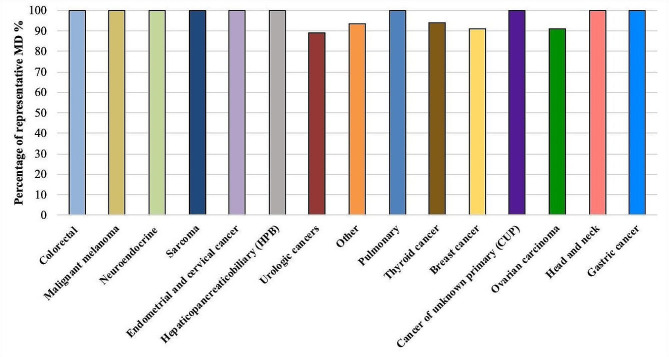
262 patients with different solid malignancies were included. 177 patients (68%) had MD and 85 (32%) had non-measurable disease (NMD) at the time point of MTB presentation in accordance with RECIST v1.1. MD was not representative of the overall tumor burden in eleven patients (6%). The main reasons for NMD were lesions with longest diameter shorter than 10 mm (22%) and non-measurable peritoneal carcinomatosis (18%). Colorectal cancer and malignant melanoma displayed the highest rates of MD (> 75%). In contrast, gastric cancer, head and neck malignancies, and ovarian carcinoma had the lowest rates of MD (< 55%). In case of MD, the measurable lesions were representative of the overall tumor burden in the vast majority of cases (94%).
Approximately one third of cancer patients with advanced solid malignancies are not eligible for treatment response assessment in trials with endpoints ORR or DOR at the time of MTB presentation. The rate of patients eligible for trials with imaging endpoints differs significantly based on the underlying malignancy and should be taken under consideration during the planning of new precision oncology trials.
评估在大型精准肿瘤中心的分子肿瘤委员会(MTB)就诊的晚期或复发性实体恶性肿瘤患者是否有资格参加以客观缓解率(ORR)或缓解持续时间(DOR)为终点的试验,这些患者的入组标准是基于实体瘤反应评估标准(RECIST 版本 1.1)有可测量的疾病(MD)。
前瞻性纳入 MTB 就诊时有可用影像学资料的患者。根据 RECIST v1.1 评估影像学数据是否存在可测量的 MD。此外,我们还评估了 MD 患者中,确定的可测量病变与总体肿瘤负担的代表性。
共纳入 262 例不同实体恶性肿瘤患者。177 例(68%)患者根据 RECIST v1.1 在 MTB 就诊时存在 MD,85 例(32%)存在不可测量的疾病(NMD)。11 例(6%)患者的 MD 不能代表总体肿瘤负担。NMD 的主要原因是最长直径小于 10mm 的病变(22%)和不可测量的腹膜癌病(18%)。结直肠癌和恶性黑色素瘤的 MD 发生率最高(>75%)。相比之下,胃癌、头颈部恶性肿瘤和卵巢癌的 MD 发生率最低(<55%)。在 MD 的情况下,可测量的病变在绝大多数情况下能代表总体肿瘤负担(94%)。
大约三分之一的晚期实体恶性肿瘤患者在 MTB 就诊时不符合以 ORR 或 DOR 为终点的试验治疗反应评估的条件。符合影像学终点试验的患者比例因基础恶性肿瘤而异,在规划新的精准肿瘤学试验时应加以考虑。