Clark Amy, Cannings-John Rebecca, Carrol Enitan D, Thomas-Jones Emma, Sefton Gerri, Hay Alastair D, Butler Christopher C, Hughes Kathryn
Paediatrics, Cambridge University Hospitals NHS Foundation Trust, Cambridge.
Centre for Trials Research, Cardiff University, Cardiff.
Br J Gen Pract. 2025 Jan 30;75(751):e98-e104. doi: 10.3399/BJGP.2023.0638. Print 2025 Feb.
Clinical tools are needed in general practice to help identify children who are seriously ill. The Liverpool quick Sequential Organ Failure Assessment (LqSOFA) was validated in an emergency department and performed well. The National Paediatric Early Warning System (PEWS) has been introduced in hospitals throughout England with hopes for implementation in general practice.
To validate the LqSOFA and National PEWS in general practice.
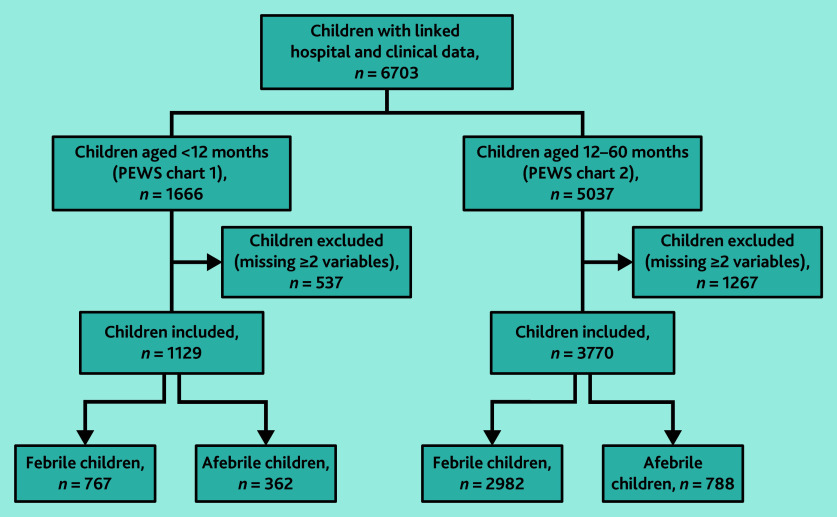
Secondary analysis of 6703 children aged <5 years presenting to 225 general practices in England and Wales with acute illnesses, linked to hospital data.
Variables from the LqSOFA and National PEWS were mapped onto study data to calculate score totals. A primary outcome of admission within 2 days of GP consultation was used to calculate sensitivity, specificity, negative predictive values (NPVs), positive predictive values (PPVs), and area under the receiver operating characteristic curve (AUC).
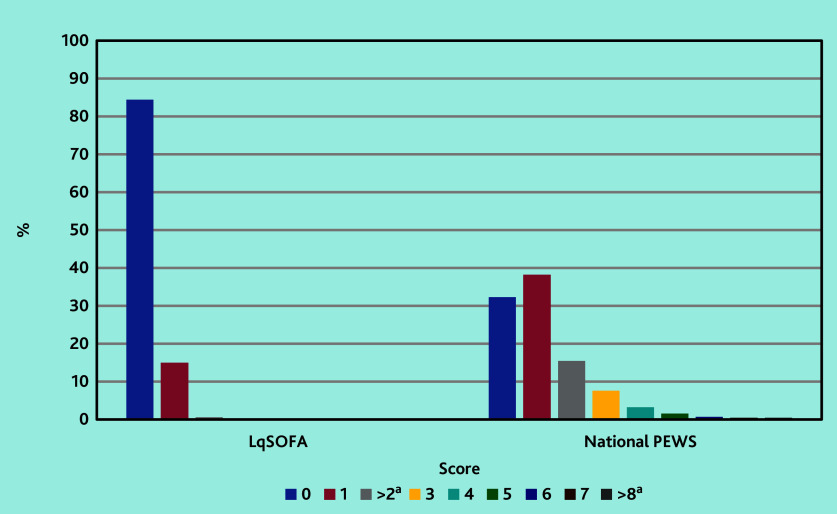
A total of 104/6703 children were admitted to hospital within 2 days (pre-test probability 1.6%) of GP consultation. The sensitivity of the LqSOFA was 30.6% (95% confidence interval [CI] = 21.8% to 41.0%), with a specificity of 84.7% (95% CI = 83.7% to 85.6%), PPV of 3.0% (95% CI = 2.1% to 4.4%), NPV of 98.7% (95% CI = 98.4% to 99.0%), and AUC of 0.58 (95% CI = 0.53 to 0.63). The sensitivity of the National PEWS was 81.0% (95% CI = 71.0% to 88.1%), with a specificity of 32.5% (95% CI = 31.2% to 33.8%), PPV of 1.9% (95% CI = 1.5% to 2.5%), NPV of 99.1% (95% CI = 98.4% to 99.4%), and AUC of 0.66 (95% CI = 0.59 to 0.72).
Although the NPVs appear useful, owing to low pre-test probabilities rather than discriminative ability, neither tool accurately identified admissions to hospital. Unconsidered use by GPs could result in unsustainable referrals.
全科医疗需要临床工具来帮助识别重症儿童。利物浦快速序贯器官衰竭评估(LqSOFA)在急诊科得到验证且表现良好。全英国的医院都引入了国家儿科早期预警系统(PEWS),并有望在全科医疗中实施。
在全科医疗中验证LqSOFA和国家PEWS。
对6703名年龄小于5岁、因急性疾病就诊于英格兰和威尔士225家全科诊所的儿童进行二次分析,并与医院数据相联系。
将LqSOFA和国家PEWS中的变量映射到研究数据上以计算总分。以全科医生会诊后2天内入院作为主要结局,计算敏感度、特异度、阴性预测值(NPV)、阳性预测值(PPV)以及受试者工作特征曲线下面积(AUC)。
共有104/6703名儿童在全科医生会诊后2天内入院(预检概率为1.6%)。LqSOFA的敏感度为30.6%(95%置信区间[CI]=21.8%至41.0%),特异度为84.7%(95%CI=83.7%至85.6%),PPV为3.0%(95%CI=2.1%至4.4%),NPV为98.7%(95%CI=98.4%至99.0%),AUC为0.58(95%CI=0.53至0.63)。国家PEWS的敏感度为81.0%(95%CI=71.0%至88.1%),特异度为32.5%(95%CI=31.2%至33.8%),PPV为1.9%(95%CI=1.5%至2.5%),NPV为99.1%(95%CI=98.4%至99.4%),AUC为0.66(95%CI=0.59至0.72)。
尽管NPV看起来有用,但由于预检概率低而非判别能力,这两种工具都不能准确识别入院情况。全科医生未经考虑的使用可能导致不可持续的转诊。