Hou Jun, Du Hui, Wang Chun, Song Fangbin, Qu Xinfeng, Wu Ruifang
Department of Obstetrics and Gynecology, Peking University Shenzhen Hospital, Shenzhen, China.
Institute of Obstetrics and Gynecology, Shenzhen Peking University-Hongkong University of Science and Technology (PKU-HKUST) Medical Center, Shenzhen, China.
Front Oncol. 2024 May 28;14:1332172. doi: 10.3389/fonc.2024.1332172. eCollection 2024.
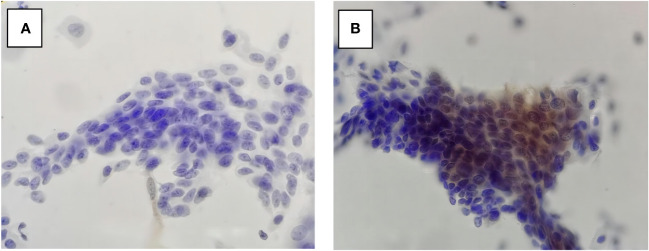
Few articles have focused on the cytological misinterpretation of high-grade squamous intraepithelial lesion (HSIL). Due to estrogen deficiency, cervical epithelial cells in postmenopausal women tend to show atrophic change that looks like HSIL on Papanicolaou-stained cytology slides, resulting in a higher rate of cytological misinterpretation. P16 immunocytochemical staining (P16 cytology) can effectively differentiate diseased cells from normal atrophic ones with less dependence on cell morphology.
To evaluate the role of P16 cytology in differentiating cytology HSIL from benign atrophy in women aged 50 years and above.
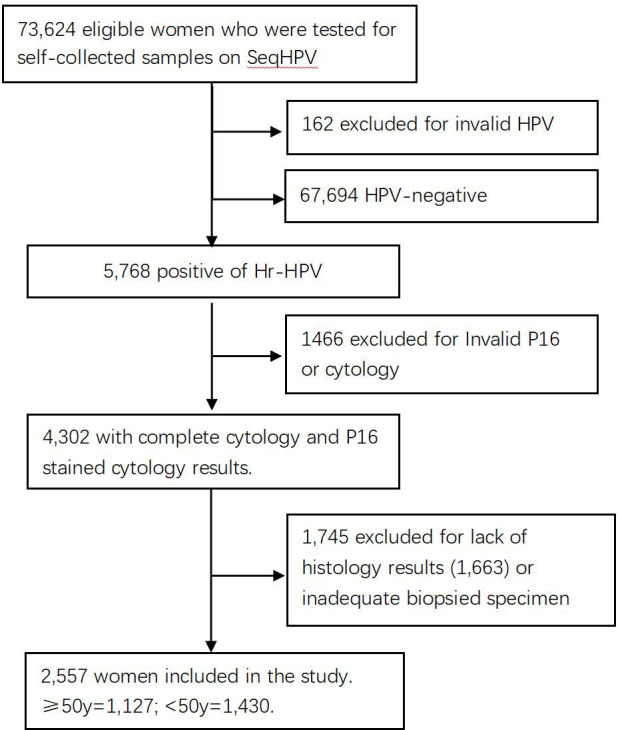
Included in this analysis were women in a cervical cancer screening project conducted in central China who tested positive for high-risk human papillomavirus (hr-HPV) and returned back for triage with complete data of primary HPV testing, liquid-based cytology (LBC) analysis, P16 immuno-stained cytology interpretation, and pathology diagnosis. The included patients were grouped by age: ≥50 (1,127 cases) and <50 years (1,430 cases). The accuracy of LBC and P16 cytology in the detection of pathology ≥HSIL was compared between the two groups, and the role of P16 immuno-stain in differentiating benign cervical lesions from cytology ≥HSIL was further analyzed.
One hundred sixty-seven women (14.8%; 167/1,127) in the ≥50 group and 255 (17.8%, 255/1,430) in the <50 group were pathologically diagnosed as HSIL (Path-HSIL). LBC [≥Atypical Squamous Cell Of Undetermined Significance (ASCUS)] and P16 cytology (positive) respectively detected 63.9% (163/255) and 90.2% (230/255) of the Path-≥HSIL cases in the <50 group and 74.3% (124/167) and 93.4% (124/167) of the Path-≥HSIL cases in the ≥50 group. LBC matched with pathology in 105 (41.2%) of the 255 Path-≥HSIL cases in the <50 group and 93 (55.7%) of the 167 Path-≥HSIL cases in the ≥50 group. There were five in the <50 group and 14 in the ≥50 group that were Path-≤LSIL cases, which were interpreted by LBC as HSIL, but negative in P16 cytology.
P16 cytology facilitates differentiation of Path-≤LSIL from LBC-≥HSIL for women 50 years of age and above. It can be used in the lower-resource areas, where qualified cytologists are insufficient, as the secondary screening test for women aged ≥50 to avoid unnecessary biopsies and misinterpretation of LBC primary or secondary screening.
很少有文章关注高级别鳞状上皮内病变(HSIL)的细胞学误诊。由于雌激素缺乏,绝经后女性的宫颈上皮细胞往往会出现萎缩性改变,在巴氏染色的细胞学涂片上看起来像HSIL,导致细胞学误诊率较高。P16免疫细胞化学染色(P16细胞学)可以有效地区分病变细胞与正常萎缩细胞,对细胞形态的依赖性较小。
评估P16细胞学在50岁及以上女性中将细胞学HSIL与良性萎缩相鉴别的作用。
纳入中国中部一项宫颈癌筛查项目中的女性,这些女性高危型人乳头瘤病毒(hr-HPV)检测呈阳性,并返回进行分流,具备初级HPV检测、液基细胞学(LBC)分析、P16免疫染色细胞学解读和病理诊断的完整数据。纳入的患者按年龄分组:≥50岁(1127例)和<50岁(1430例)。比较两组中LBC和P16细胞学检测病理学≥HSIL的准确性,并进一步分析P16免疫染色在将良性宫颈病变与细胞学≥HSIL相鉴别中的作用。
≥50岁组中有167名女性(14.8%;167/1127),<50岁组中有(255)名女性(17.8%,255/1430)经病理诊断为HSIL(病理HSIL)。LBC[≥意义不明确的非典型鳞状细胞(ASCUS)]和P16细胞学(阳性)分别在<50岁组中检测到255例病理≥HSIL病例中的63.9%(163/255)和90.2%(230/255),在≥50岁组中检测到167例病理≥HSIL病例中的74.3%(124/167)和93.4%(124/167)。在<50岁组的255例病理≥HSIL病例中,LBC与病理相符的有105例(41.2%),在≥50岁组的167例病理≥HSIL病例中,LBC与病理相符的有93例(55.7%)。<50岁组中有5例,≥50岁组中有14例为病理≤低级别鳞状上皮内病变(LSIL)病例,LBC将其解读为HSIL,但P16细胞学为阴性。
P16细胞学有助于50岁及以上女性将病理≤LSIL与LBC≥HSIL相鉴别。在合格细胞病理学家不足的资源匮乏地区,它可作为≥50岁女性的二次筛查试验,以避免不必要的活检以及LBC初次或二次筛查的误诊。