Laing Don, Walsh Eamon P G, Alsweiler Jane M, Hanning Sara M, Meyer Michael P, Ardern Julena, Cutfield Wayne S, Rogers Jenny, Gamble Gregory D, Chase J Geoffrey, Harding Jane E, McKinlay Christopher J D
Liggins Institute, University of Auckland, Auckland, New Zealand.
Department of Paediatrics: Child and Youth Health, University of Auckland, Auckland, New Zealand.
JAMA Netw Open. 2024 Jun 3;7(6):e2415764. doi: 10.1001/jamanetworkopen.2024.15764.
Neonatal hypoglycemia is an important preventable cause of neurodevelopmental impairment, but there is a paucity of evidence to guide treatment.
To evaluate whether early, low-dose oral diazoxide for severe or recurrent neonatal hypoglycemia reduces time to resolution of hypoglycemia.
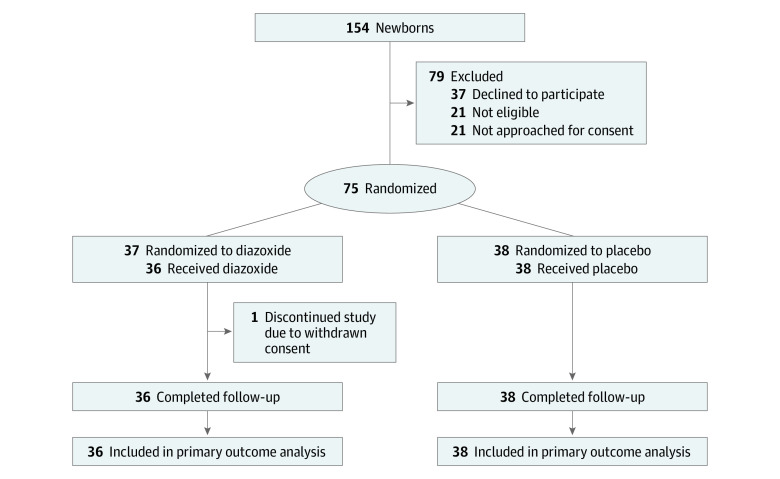
DESIGN, SETTING, AND PARTICIPANTS: This 2-arm, placebo-controlled randomized clinical trial was conducted from May 2020 to February 2023 in tertiary neonatal units at 2 New Zealand hospitals. Participants were neonates born at 35 or more weeks' gestation and less than 1 week of age with severe hypoglycemia (blood glucose concentration <22 mg/dL or <36 mg/dL despite 2 doses of dextrose gel) or recurrent hypoglycemia (≥3 episodes of a blood glucose concentration <47 mg/dL within 48 hours).
Newborns were randomized 1:1 to receive diazoxide suspension (loading dose, 5 mg/kg; maintenance, 1.5 mg/kg every 12 hours) or placebo, titrated per protocol.
The primary outcome was time to resolution of hypoglycemia, defined as enteral bolus feeding without intravenous fluids and normoglycemia (blood glucose concentration of 47-98 mg/dL) for at least 24 hours, compared between groups using adjusted Cox proportional hazards regression. Hazard ratios adjusted for stratification variables and gestation length are reported. Prespecified secondary outcomes, including number of blood glucose tests and episodes of hypoglycemia, duration of hypoglycemia, and time to enteral bolus feeding and weaning from intravenous fluids, were compared by generalized linear models. Newborns were followed up for at least 2 weeks.
Of 154 newborns screened, 75 were randomized and 74 with evaluable data were included in the analysis (mean [SD] gestational age for the full cohort, 37.6 [1.6] weeks), 36 in the diazoxide group and 38 in the placebo group. Baseline characteristics were similar: in the diazoxide group, mean (SD) gestational age was 37.9 (1.6) weeks and 26 (72%) were male; in the placebo group, mean (SD) gestational age was 37.4 (1.5) weeks and 27 (71%) were male. There was no significant difference in time to resolution of hypoglycemia (adjusted hazard ratio [AHR], 1.39; 95% CI, 0.84-2.23), possibly due to increased episodes of elevated blood glucose concentration and longer time to normoglycemia in the diazoxide group. Resolution of hypoglycemia, when redefined post hoc as enteral bolus feeding without intravenous fluids for at least 24 hours with no further hypoglycemia, was reached by more newborns in the diazoxide group (AHR, 2.60; 95% CI, 1.53-4.46). Newborns in the diazoxide group had fewer blood glucose tests (adjusted count ratio [ACR], 0.63; 95% CI, 0.56-0.71) and episodes of hypoglycemia (ACR, 0.32; 95% CI, 0.17-0.63), reduced duration of hypoglycemia (adjusted ratio of geometric means [ARGM], 0.18; 95% CI, 0.06-0.53), and reduced time to enteral bolus feeding (ARGM, 0.74; 95% CI, 0.58-0.95) and weaning from intravenous fluids (ARGM, 0.72; 95% CI, 0.60-0.87). Only 2 newborns (6%) treated with diazoxide had hypoglycemia after the loading dose compared with 20 (53%) with placebo.
In this randomized clinical trial, early treatment of severe or recurrent neonatal hypoglycemia with low-dose oral diazoxide did not reduce time to resolution of hypoglycemia but reduced time to enteral bolus feeding and weaning from intravenous fluids, duration of hypoglycemia, and frequency of blood glucose testing compared with placebo.
ANZCTR.org.au Identifier: ACTRN12620000129987.
新生儿低血糖是神经发育障碍的一个重要可预防原因,但指导治疗的证据不足。
评估早期、低剂量口服二氮嗪治疗严重或复发性新生儿低血糖是否能缩短低血糖缓解时间。
设计、地点和参与者:这项双臂、安慰剂对照的随机临床试验于2020年5月至2023年2月在新西兰2家医院的三级新生儿病房进行。参与者为孕周35周及以上、年龄小于1周的新生儿,患有严重低血糖(血糖浓度<22mg/dL或尽管使用了2剂葡萄糖凝胶但血糖浓度仍<36mg/dL)或复发性低血糖(48小时内血糖浓度<47mg/dL发作≥3次)。
新生儿按1:1随机分组,接受二氮嗪混悬液(负荷剂量,5mg/kg;维持剂量,每12小时1.5mg/kg)或安慰剂,按方案进行滴定。
主要结局是低血糖缓解时间,定义为在不使用静脉输液且血糖正常(血糖浓度为47 - 98mg/dL)的情况下进行肠内推注喂养至少24小时,使用调整后的Cox比例风险回归比较两组。报告经分层变量和孕周调整后的风险比。通过广义线性模型比较预先设定的次要结局,包括血糖检测次数和低血糖发作次数、低血糖持续时间以及肠内推注喂养时间和停止静脉输液时间。对新生儿进行至少2周的随访。
在154名筛查的新生儿中,75名被随机分组,74名有可评估数据的新生儿纳入分析(整个队列的平均[标准差]孕周为37.6[1.6]周),二氮嗪组36名,安慰剂组38名。基线特征相似:二氮嗪组平均(标准差)孕周为37.9(1.6)周,26名(72%)为男性;安慰剂组平均(标准差)孕周为(1.5)周,27名(71%)为男性。低血糖缓解时间无显著差异(调整后风险比[AHR],1.39;95%置信区间,0.84 - 2.23),可能是由于二氮嗪组血糖浓度升高发作次数增加和达到正常血糖的时间延长。在事后将低血糖缓解重新定义为在不使用静脉输液的情况下进行肠内推注喂养至少24小时且无进一步低血糖时,二氮嗪组更多新生儿达到缓解(AHR,2.60;95%置信区间,1.53 - 4.46)。二氮嗪组新生儿的血糖检测次数(调整后计数比[ACR],0.63;95%置信区间,0.56 - 0.71)和低血糖发作次数(ACR,0.32;95%置信区间,0.17 - 0.63)减少,低血糖持续时间缩短(调整后几何均数比[ARGM],0.18;95%置信区间,0.06 - 0.53),肠内推注喂养时间(ARGM,0.74;95%置信区间,0.58 - 0.95)和停止静脉输液时间(ARGM,0.72;95%置信区间,0.60 - 0.87)缩短。与安慰剂组的20名(53%)相比,仅2名(6%)接受二氮嗪治疗的新生儿在负荷剂量后出现低血糖。
在这项随机临床试验中,早期用低剂量口服二氮嗪治疗严重或复发性新生儿低血糖并未缩短低血糖缓解时间,但与安慰剂相比,缩短了肠内推注喂养时间和停止静脉输液时间、低血糖持续时间以及血糖检测频率。
ANZCTR.org.au标识符:ACTRN12620000129987。