Department of Surgery, Obihiro Kosei General Hospital, West 14 South 10, Obihiro, Hokkaido, 080-0024, Japan.
Department of Thoracic Surgery, Hokkaido University Hospital, West 5 North 14, Kita-Ku, Sapporo, Hokkaido, 060-8648, Japan.
J Med Case Rep. 2024 Jun 16;18(1):280. doi: 10.1186/s13256-024-04602-3.
Intercostal artery bleeding often occurs in a single vessel; in rare cases, it can occur in numerous vessels, making it more difficult to manage.
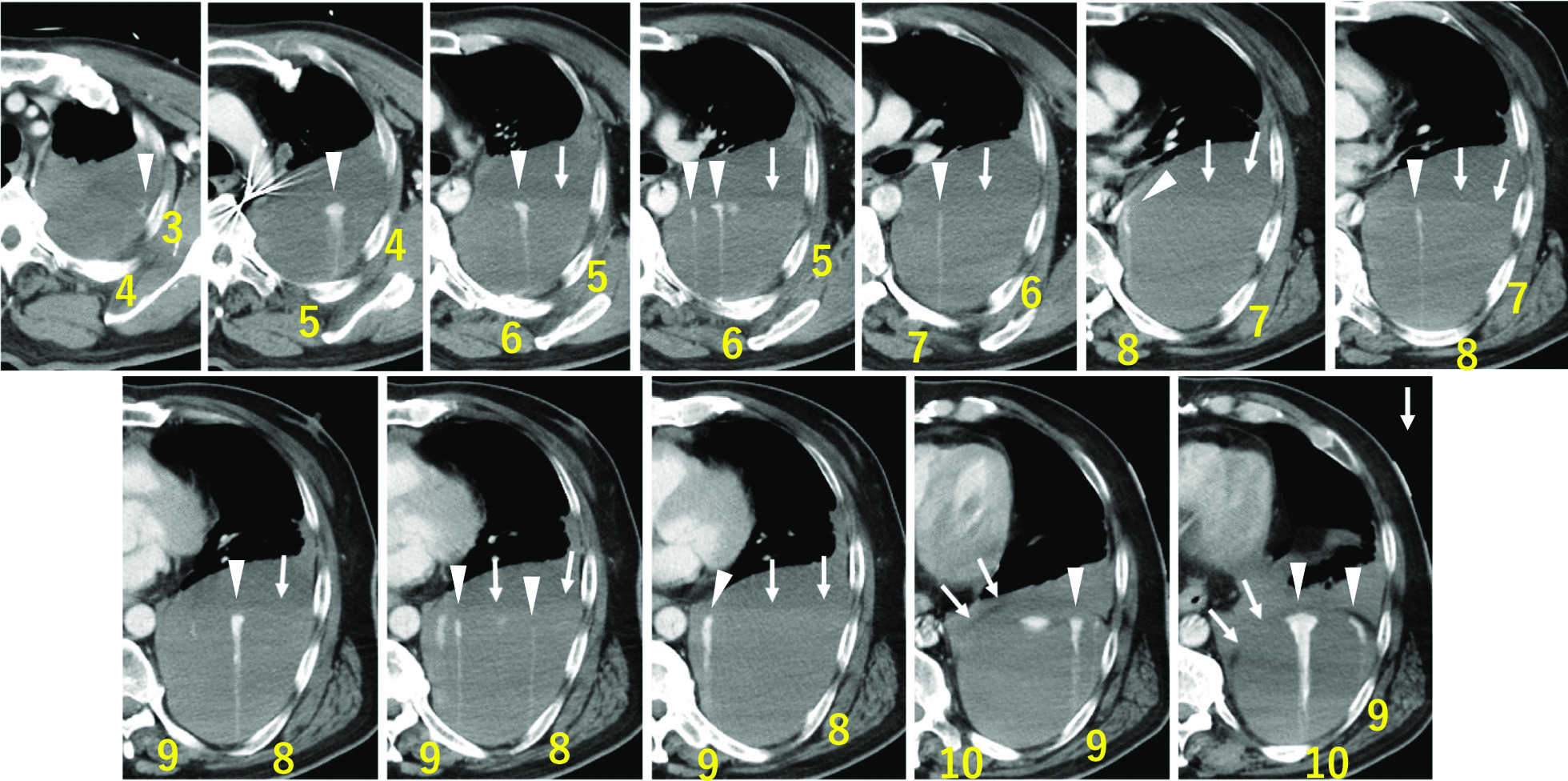
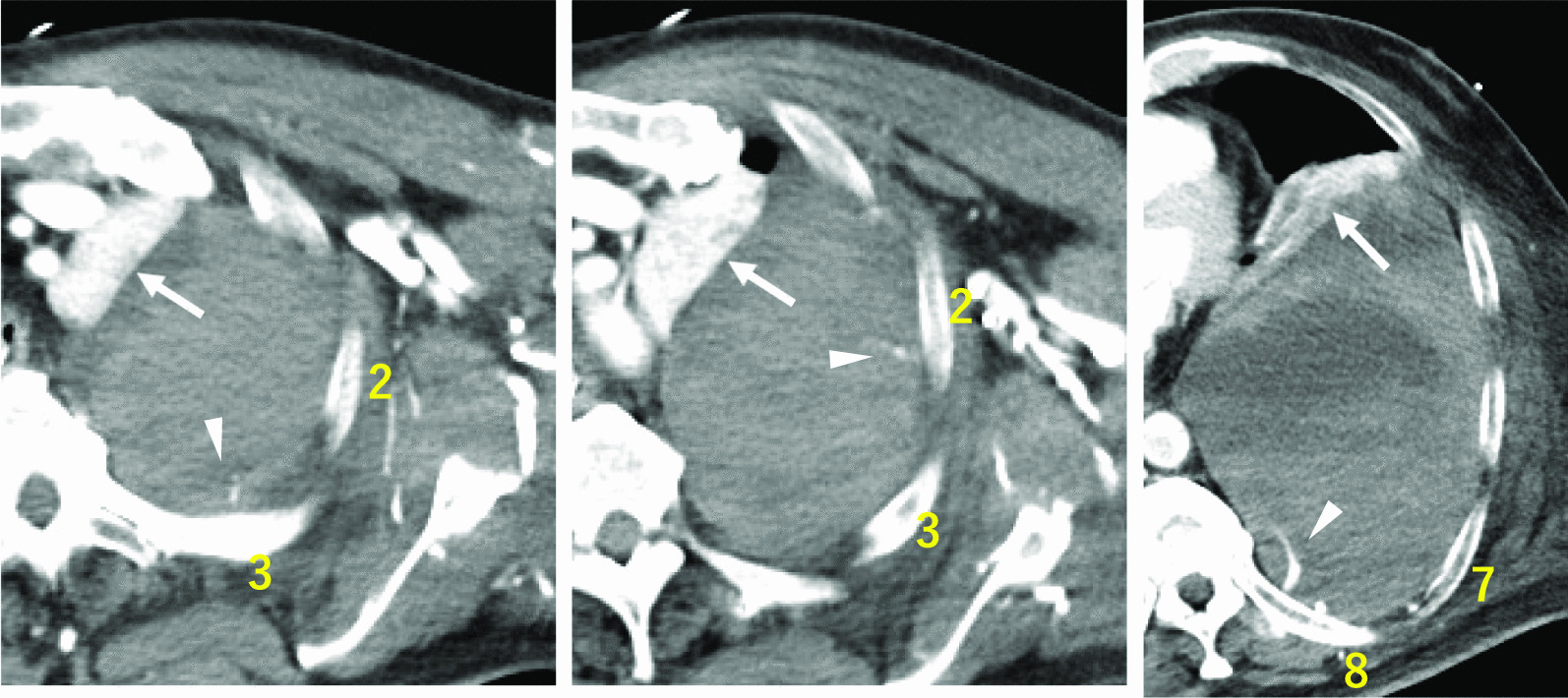
A 63-year-old Japanese man was admitted to the emergency department owing to sudden chest and back pain, dizziness, and nausea. Emergency coronary angiography revealed myocardial infarction secondary to right coronary artery occlusion. After intra-aortic balloon pumping, percutaneous coronary intervention was performed in the right coronary artery. At 12 hours following percutaneous coronary intervention, the patient developed new-onset left anterior chest pain and hypotension. Contrast-enhanced computed tomography revealed 15 sites of contrast extravasation within a massive left extrapleural hematoma. Emergency angiography revealed contrast leakage in the left 6th to 11th intercostal arteries; hence, transcatheter arterial embolization was performed. At 2 days after transcatheter arterial embolization, his blood pressure subsequently decreased, and contrast-enhanced computed tomography revealed the re-enlargement of extrapleural hematoma with multiple sites of contrast extravasation. Emergency surgery was performed owing to persistent bleeding. No active arterial hemorrhage was observed intraoperatively. Bleeding was observed in various areas of the chest wall, and an oxidized cellulose membrane was applied following ablation and hemostasis. The postoperative course was uneventful.
We report a case of spontaneous intercostal artery bleeding occurring simultaneously in numerous vessels during antithrombotic therapy with mechanical circulatory support that was difficult to manage. As bleeding from numerous vessels may occur during antithrombotic therapy, even without trauma, appropriate treatments, such as transcatheter arterial embolization and surgery, should be selected in patients with such cases.
肋间动脉出血通常发生在单一血管中;在极少数情况下,它可能发生在多个血管中,这使得处理更加困难。
一名 63 岁的日本男性因突发胸痛、背痛、头晕和恶心而被收入急诊部。紧急冠状动脉造影显示右冠状动脉闭塞引起的心肌梗死。在主动脉内球囊泵后,对右冠状动脉进行了经皮冠状动脉介入治疗。在经皮冠状动脉介入治疗后 12 小时,患者出现新发左前胸疼痛和低血压。增强 CT 显示巨大左胸外血肿内有 15 个造影剂外渗部位。紧急血管造影显示左第 6 至 11 肋间动脉有造影剂渗漏;因此,进行了经导管动脉栓塞术。在经导管动脉栓塞术后 2 天,他的血压随后下降,增强 CT 显示胸外血肿再次扩大,有多个造影剂外渗部位。由于持续出血,进行了紧急手术。术中未观察到活跃的动脉出血。在胸腔壁的各个部位观察到出血,并在消融和止血后应用氧化纤维素膜。术后过程平稳。
我们报告了一例在机械循环支持的抗栓治疗期间同时发生在多个血管的自发性肋间动脉出血的病例,处理困难。由于在抗栓治疗期间即使没有外伤也可能发生多支血管出血,对于此类病例应选择适当的治疗方法,如经导管动脉栓塞术和手术。