Núcleo de Pesquisa Clínica, Hospital do Cancer III, Instituto Nacional de Câncer -, Rio de Janeiro 20560-121, Brazil.
School of Biosciences, Faculty of Health and Medical Sciences, University of Surrey, Guilford GU2 7XH, UK.
Int J Mol Sci. 2024 May 27;25(11):5825. doi: 10.3390/ijms25115825.
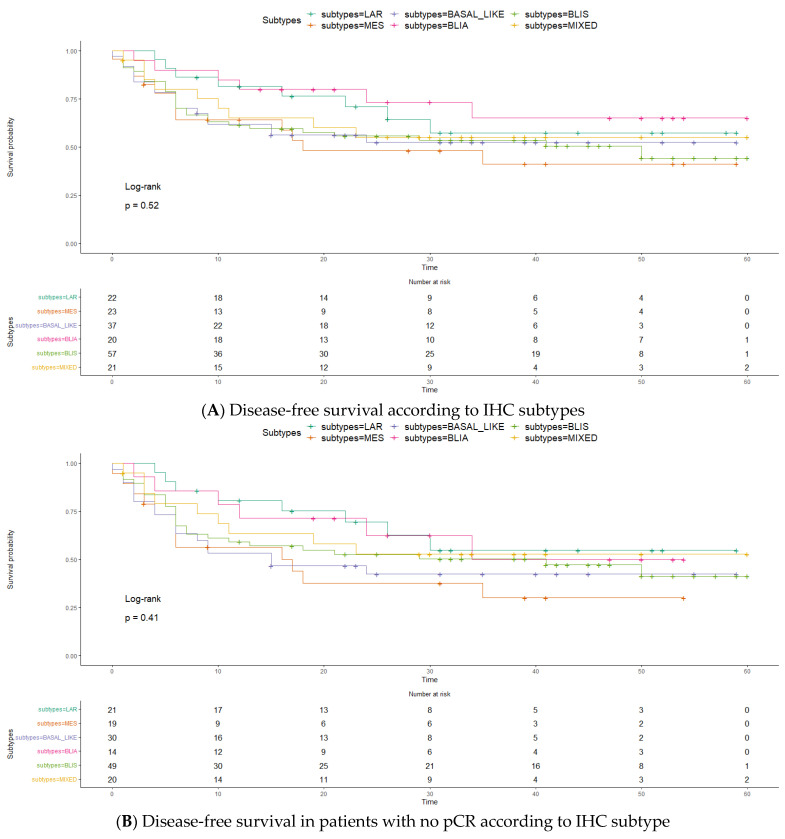
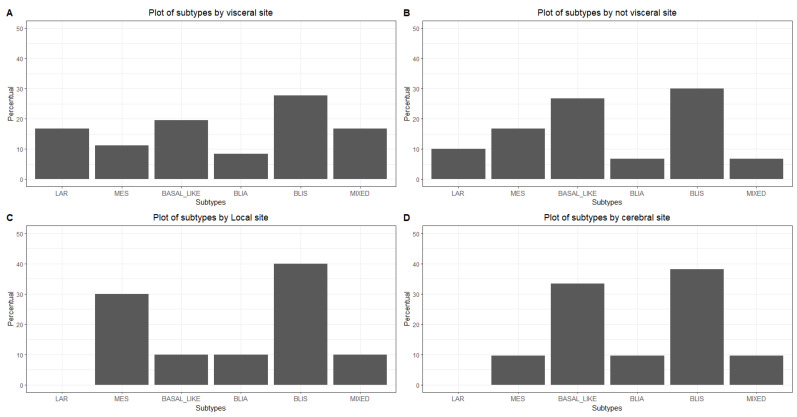
The intrinsic subtype of triple-negative breast cancer (TNBC) is based on genomic evaluation. In this study, we report the survival and pathological complete response (pCR) rates of TNBC patients subtyped by IHC and treated with neoadjuvant chemotherapy (NACT). A retrospective cohort of 187 TNBC patients who received NACT between 2008 and 2017 was used, and IHC subtyping was performed on biopsy specimens before chemotherapy. The subtyping revealed predominantly basal-like tumors (IHC-BL, 61%), followed by basal-like immune-suppressed tumors (IHC-BLIS, 31%), mesenchymal tumors (12.5%), luminal androgen receptor tumors (IHC-LAR, 12%), and basal-like immune-activated tumors (IHC-BLIA, 10.9%). The pCR rate varied among subtypes, with IHC-BLIA showing the highest (30.0%) and IHC-LAR showing the lowest (4.5%). IHC-BLIS led in recurrence sites. Overall and disease-free survival analyses did not show significant differences among subtypes, although IHC-BLIA demonstrated a trend toward better survival, and IHC-mesenchymal, worse. Patients who achieved pCR exhibited significantly better disease-free survival and overall survival than non-responders. This study underscores the potential of IHC-based subtyping in TNBC management, highlighting distinct response patterns to neoadjuvant chemotherapy and potential implications for treatment strategies. Further research is warranted to validate these findings and explore tailored therapeutic approaches for specific TNBC subtypes.
三阴性乳腺癌(TNBC)的内在亚型基于基因组评估。本研究报告了通过免疫组织化学(IHC)进行亚型分类并接受新辅助化疗(NACT)治疗的 TNBC 患者的生存和病理完全缓解(pCR)率。我们回顾性分析了 2008 年至 2017 年间接受 NACT 的 187 例 TNBC 患者,在化疗前对活检标本进行 IHC 亚型分类。IHC 分类结果显示,主要为基底样肿瘤(IHC-BL,61%),其次是基底样免疫抑制肿瘤(IHC-BLIS,31%)、间充质肿瘤(12.5%)、腔面雄激素受体肿瘤(IHC-LAR,12%)和基底样免疫激活肿瘤(IHC-BLIA,10.9%)。不同亚型的 pCR 率不同,IHC-BLIA 最高(30.0%),IHC-LAR 最低(4.5%)。IHC-BLIS 导致的复发部位最多。总体生存和无病生存分析显示各亚型之间无显著差异,尽管 IHC-BLIA 显示出更好的生存趋势,而 IHC-间充质型则较差。达到 pCR 的患者无病生存和总体生存明显优于无应答者。本研究强调了 IHC 为基础的 TNBC 管理中的潜在作用,突出了对新辅助化疗的不同反应模式以及对治疗策略的潜在影响。需要进一步研究来验证这些发现,并探索针对特定 TNBC 亚型的个体化治疗方法。