Cao Jian, Yu Miao, Xiao Yu, Dong Ran, Wang Jiayang
Department of Cardiac Surgery, Beijing Institute of Heart, Lung and Blood Vessel Diseases- Beijing Anzhen Hospital, Affiliated of Capital Medical University, Beijing, China.
Front Cardiovasc Med. 2024 Jun 4;11:1398700. doi: 10.3389/fcvm.2024.1398700. eCollection 2024.
Ischaemic heart failure with reduced ejection fraction (HFrEF) caused by coronary artery disease accounts for the largest proportion of heart failure cases with the worst prognosis. Coronary artery bypass grafting (CABG) is the most effective treatment for ischaemic HFrEF. On-pump and off-pump are the two surgical methods used for CABG. Whether patients with HFrEF should undergo on- or off-pump CABG is controversial in coronary heart disease surgery. The left ventricular end-systolic volume index (LVSEVI) is the gold standard for evaluating the severity of left ventricular remodelling; however, its effect on the perioperative risk and long-term survival rate of patients with HFrEF undergoing CABG remains unclear.
This single centre prospective cohort analysis included 118 coronary heart disease patients with symptoms and signs of heart failure and a left ventricular ejection fraction (LVEF) of <40% who were enrolled consecutively from January 2019 to December 2023. Operative mortality, perioperative complications, and long-term survival were compared among patients treated with various LVESVIs and surgical methods. The primary outcomes were cardiac death, myocardial infarction, heart failure, stroke, and revascularization, (percutaneous coronary intervention or redo CABG) with a median follow-up of 38 ± 10 months.
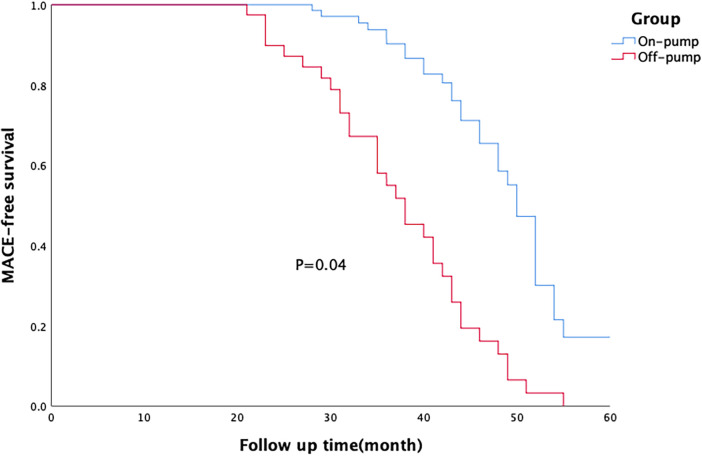
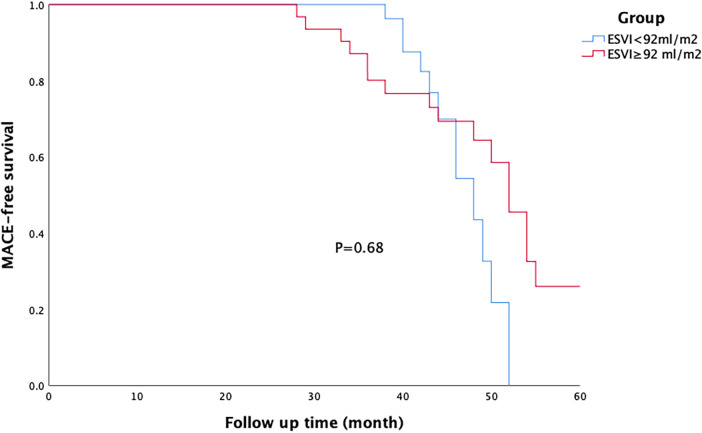
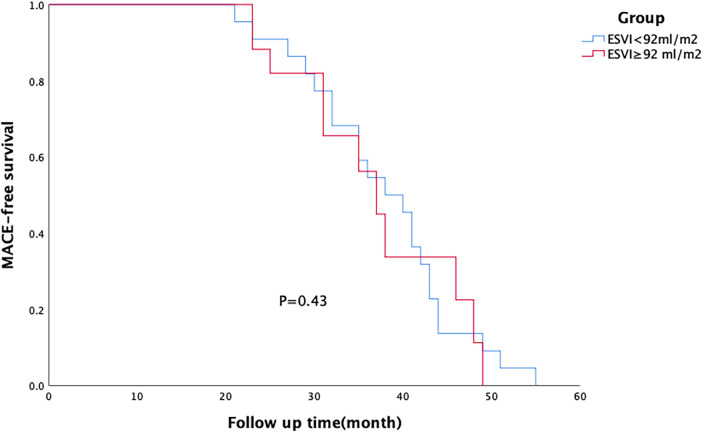
The 30-day postoperative mortality of 118 patients was 6.8%. Patients in the off-pump group had significantly higher perioperative mortality than those in the on-pump group (12.5% vs. 3.8%, = 0.03). In the off-pump group, a higher proportion of patients required perioperative mechanical assistance, such as intra-aortic artery balloon pump (IABP) or extracorporeal membrane oxygenation (ECMO), compared to those in the on-pump group (IABP: 75% vs. 47.4%, = 0.004; ECMO: 22.5% vs. 1.3%, = 0.000). Patients in the off-pump group were more likely to have postoperative atrial fibrillation (AF) (35% vs. 14.1%, = 0.01). In the on-pump group, the incidence of postoperative AF (25% vs. 6.5%, = 0.02) and IABP use (62.5% vs. 36.9%, = 0.03) were significantly higher in patients with more severe left ventricular remodelling than in those with less severe left ventricular remodelling. In the off-pump group, patients with more severe left ventricular remodelling had higher ECMO usage (38.9% vs. 9.1%, = 0.04), incidence of postoperative AF (61.1% vs. 13.6%, = 0.02), and perioperative mortality (22.2%). Major adverse cardiac event (MACE)-free survival rate was significantly higher in the on-pump group than in the off-pump group, and there was no significant difference in MACE free survival rates between the two groups of patients with different degrees of left ventricular remodelling.
On-pump bypass is a better surgical procedure for patients with ischaemic HFrEF, especially those with severe left ventricular remodelling. Left ventricular remodelling increases perioperative mortality but has no effect on long-term survival.
由冠状动脉疾病引起的射血分数降低的缺血性心力衰竭(HFrEF)在心力衰竭病例中占比最大,预后最差。冠状动脉旁路移植术(CABG)是治疗缺血性HFrEF最有效的方法。体外循环下和非体外循环下是CABG使用的两种手术方式。在冠心病手术中,HFrEF患者应接受体外循环下还是非体外循环下CABG存在争议。左心室收缩末期容积指数(LVSEVI)是评估左心室重构严重程度的金标准;然而,其对接受CABG的HFrEF患者围手术期风险和长期生存率的影响仍不明确。
这项单中心前瞻性队列分析纳入了2019年1月至2023年12月连续入选的118例有心力衰竭症状和体征且左心室射血分数(LVEF)<40%的冠心病患者。比较了不同LVSEVI和手术方式治疗的患者的手术死亡率、围手术期并发症和长期生存率。主要结局为心源性死亡、心肌梗死、心力衰竭、中风和血运重建(经皮冠状动脉介入治疗或再次CABG),中位随访时间为38±10个月。
118例患者术后30天死亡率为6.8%。非体外循环组患者围手术期死亡率显著高于体外循环组(12.5%对3.8%,P=0.03)。与体外循环组相比,非体外循环组中需要围手术期机械辅助的患者比例更高,如主动脉内球囊反搏(IABP)或体外膜肺氧合(ECMO)(IABP:75%对47.4%,P=0.004;ECMO:22.5%对1.3%,P=0.000)。非体外循环组患者术后房颤(AF)发生率更高(35%对14.1%,P=0.01)。在体外循环组中,左心室重构更严重的患者术后AF发生率(25%对6.5%,P=0.02)和IABP使用率(62.5%对36.9%,P=0.03)显著高于左心室重构较轻的患者。在非体外循环组中,左心室重构更严重的患者ECMO使用率更高(38.9%对9.1%,P=0.04)、术后AF发生率更高(61.1%对13.6%,P=0.02)以及围手术期死亡率更高(22.2%)。体外循环组无主要不良心脏事件(MACE)生存率显著高于非体外循环组,不同程度左心室重构的两组患者MACE无事件生存率无显著差异。
体外循环下搭桥术对于缺血性HFrEF患者,尤其是左心室重构严重的患者是一种更好的手术方式。左心室重构会增加围手术期死亡率,但对长期生存无影响。