Chai Audrey L, Rakočević Rastko, El-Baba Firas M, Killu Keith
Department of Medicine, University of Southern California, Los Angeles, USA.
Division of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, University of Southern California, Los Angeles, USA.
Cureus. 2024 May 28;16(5):e61253. doi: 10.7759/cureus.61253. eCollection 2024 May.
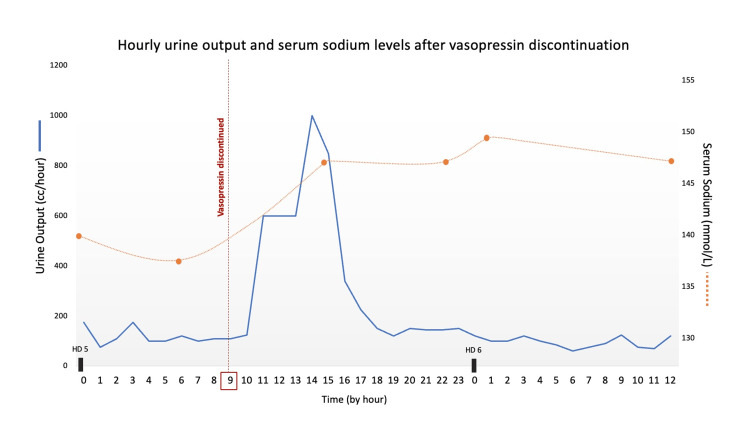
Vasopressin infusion is commonly used in intensive care settings during states of advanced vasodilatory shock for its vasoconstrictive properties. Vasopressin also acts on renal tubular cell receptors in the collecting ducts of kidneys to allow for water reabsorption. The sudden discontinuation of vasopressin infusion can lead to the development of transient diabetes insipidus (DI) with classic findings of polyuria, dilute urine, and hypernatremia. We report the case of a 59-year-old male who underwent an emergent bedside cricothyrotomy procedure secondary to papillary carcinoma of the thyroid and subsequently developed septic shock requiring initiation of vasopressin infusion for hemodynamic support. He remained on vasopressin for five days before the infusion was discontinued after clinical improvement. Within 12 hours of vasopressin discontinuation, the patient developed polyuria (> 3 L/day urine output) with volumes as high as 1 L per hour. His serum sodium levels increased more than 10 mmol/L from 137 to 149 mmol/L. This case is unique from prior reports, as our patient was without any neurological or neurosurgical comorbidities that would predispose him to an organic central cause of DI. Furthermore, the patient's large-volume diuresis and serum abnormalities spontaneously self-improved within 24 hours without significant medical intervention. In conclusion, this case adds to a growing number of reports of transient DI following vasopressin withdrawal, demonstrating the need to formally recognize this occurrence as a potential consequence of vasopressin use in intensive care settings.
在严重血管舒张性休克状态下,由于其血管收缩特性,血管加压素输注常用于重症监护环境。血管加压素还作用于肾脏集合管的肾小管细胞受体,以促进水的重吸收。突然停止血管加压素输注可导致短暂性尿崩症(DI),出现多尿、低比重尿和高钠血症等典型表现。我们报告一例59岁男性病例,该患者因甲状腺乳头状癌接受了床边紧急环甲膜切开术,随后发生感染性休克,需要启动血管加压素输注以进行血流动力学支持。在临床改善后停止输注前,他持续使用血管加压素五天。在停止血管加压素输注后的12小时内,患者出现多尿(尿量>3L/天),每小时尿量高达1L。他的血清钠水平从137mmol/L升至149mmol/L,升高超过10mmol/L。该病例与之前的报告不同,因为我们的患者没有任何神经或神经外科合并症,这些合并症会使他易患器质性中枢性尿崩症。此外,患者的大量利尿和血清异常在24小时内自发自行改善,无需重大医疗干预。总之,该病例增加了越来越多关于血管加压素撤药后短暂性尿崩症的报告,表明有必要正式认识到这种情况是重症监护环境中使用血管加压素的潜在后果。