Department of Surgery, Istanbul University, Istanbul Faculty of Medicine, Istanbul, Türkiye.
Department of Surgical Oncology, Istanbul University, Institute of Oncology, Istanbul, Türkiye.
World J Surg Oncol. 2024 Jul 6;22(1):178. doi: 10.1186/s12957-024-03413-6.
Any advantage of performing targeted axillary dissection (TAD) compared to sentinel lymph node (SLN) biopsy (SLNB) is under debate in clinically node-positive (cN+) patients diagnosed with breast cancer. Our objective was to assess the feasibility of the removal of the clipped node (RCN) with TAD or without imaging-guided localisation by SLNB to reduce the residual axillary disease in completion axillary lymph node dissection (cALND) in cN+ breast cancer.
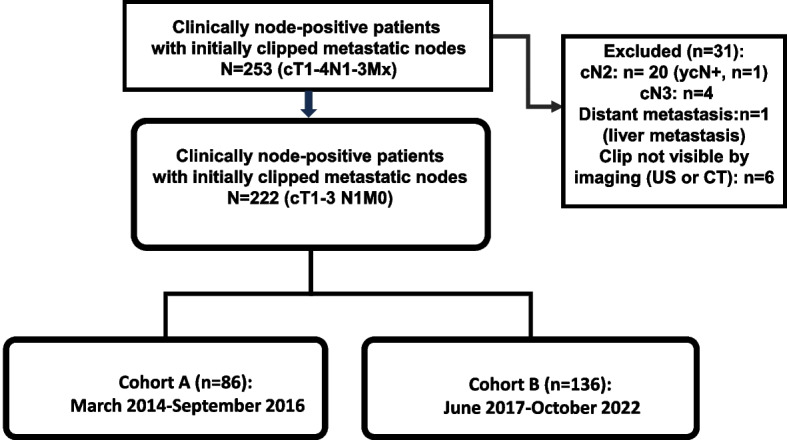
A combined analysis of two prospective cohorts, including 253 patients who underwent SLNB with/without TAD and with/without ALND following NAC, was performed. Finally, 222 patients (cT1-3N1/ycN0M0) with a clipped lymph node that was radiologically visible were analyzed.
Overall, the clipped node was successfully identified in 246 patients (97.2%) by imaging. Of 222 patients, the clipped lymph nodes were non-SLNs in 44 patients (19.8%). Of patients in cohort B (n=129) with TAD, the clipped node was successfully removed by preoperative image-guided localisation, or the clipped lymph node was removed as the SLN as detected on preoperative SPECT-CT. Among patients with ypSLN(+) (n=109), no significant difference was found in non-SLN positivity at cALND between patients with TAD and RCN (41.7% vs. 46.9%, p=0.581). In the subgroup with TAD with axillary lymph node dissection (ALND; n=60), however, patients with a lymph node (LN) ratio (LNR) less than 50% and one metastatic LN in the TAD specimen were found to have significantly decreased non-SLN positivity compared to others (27.6% vs. 54.8%, p=0.032, and 22.2% vs. 50%, p=0.046).
TAD by imaging-guided localisation is feasible with excellent identification rates of the clipped node. This approach has also been found to reduce the additional non-SLN positivity rate to encourage omitting ALND in patients with a low metastatic burden undergoing TAD.
在临床淋巴结阳性(cN+)乳腺癌患者中,与前哨淋巴结活检(SLNB)相比,行腋窝定向清扫术(TAD)是否具有优势存在争议。我们的目的是评估在接受新辅助化疗(NAC)后行 SLNB 联合 TAD 或无 SLNB 联合 TAD 时,能否通过移除夹闭的淋巴结(RCN)来减少 cN+乳腺癌患者完成腋窝淋巴结清扫(cALND)中的残余腋窝疾病。
对 253 例行 SLNB 联合/不联合 TAD 及 NAC 后行 ALND 的前瞻性队列进行联合分析。最终,对 222 例(cT1-3N1/ycN0M0 且夹闭的淋巴结在影像学上可见)存在夹闭淋巴结的患者进行了分析。
在 246 例(97.2%)患者中,通过影像学成功识别了夹闭的淋巴结。在 222 例患者中,44 例(19.8%)患者的夹闭淋巴结为非前哨淋巴结。在队列 B(n=129)中,行 TAD 的患者通过术前影像学引导定位或术前 SPECT-CT 检测到的夹闭淋巴结作为前哨淋巴结成功切除。在前哨淋巴结阳性(ypSLN(+))的患者(n=109)中,TAD 组与 RCN 组 cALND 中存在非前哨淋巴结阳性的患者比例无显著差异(41.7% vs. 46.9%,p=0.581)。然而,在 TAD 联合腋窝淋巴结清扫(ALND)的亚组(n=60)中,与其他患者相比,前哨淋巴结阳性且 TAD 标本中前哨淋巴结转移数小于 50%或仅存在 1 枚转移性淋巴结的患者,非前哨淋巴结阳性的比例显著降低(27.6% vs. 54.8%,p=0.032;22.2% vs. 50%,p=0.046)。
通过影像学引导定位行 TAD 是可行的,夹闭淋巴结的识别率很高。这种方法还可以降低非前哨淋巴结阳性率,鼓励对接受 TAD 治疗且转移负荷较低的患者省略 ALND。