Banys-Paluchowski Maggie, Gasparri Maria Luisa, de Boniface Jana, Gentilini Oreste, Stickeler Elmar, Hartmann Steffi, Thill Marc, Rubio Isabel T, Di Micco Rosa, Bonci Eduard-Alexandru, Niinikoski Laura, Kontos Michalis, Karadeniz Cakmak Guldeniz, Hauptmann Michael, Peintinger Florentia, Pinto David, Matrai Zoltan, Murawa Dawid, Kadayaprath Geeta, Dostalek Lukas, Nina Helidon, Krivorotko Petr, Classe Jean-Marc, Schlichting Ellen, Appelgren Matilda, Paluchowski Peter, Solbach Christine, Blohmer Jens-Uwe, Kühn Thorsten
Department of Obstetrics and Gynecology, Campus Lübeck, University Hospital of Schleswig Holstein, 23538 Lübeck, Germany.
Medical Faculty, Heinrich-Heine-University Düsseldorf, 40225 Düsseldorf, Germany.
Cancers (Basel). 2021 Mar 29;13(7):1565. doi: 10.3390/cancers13071565.
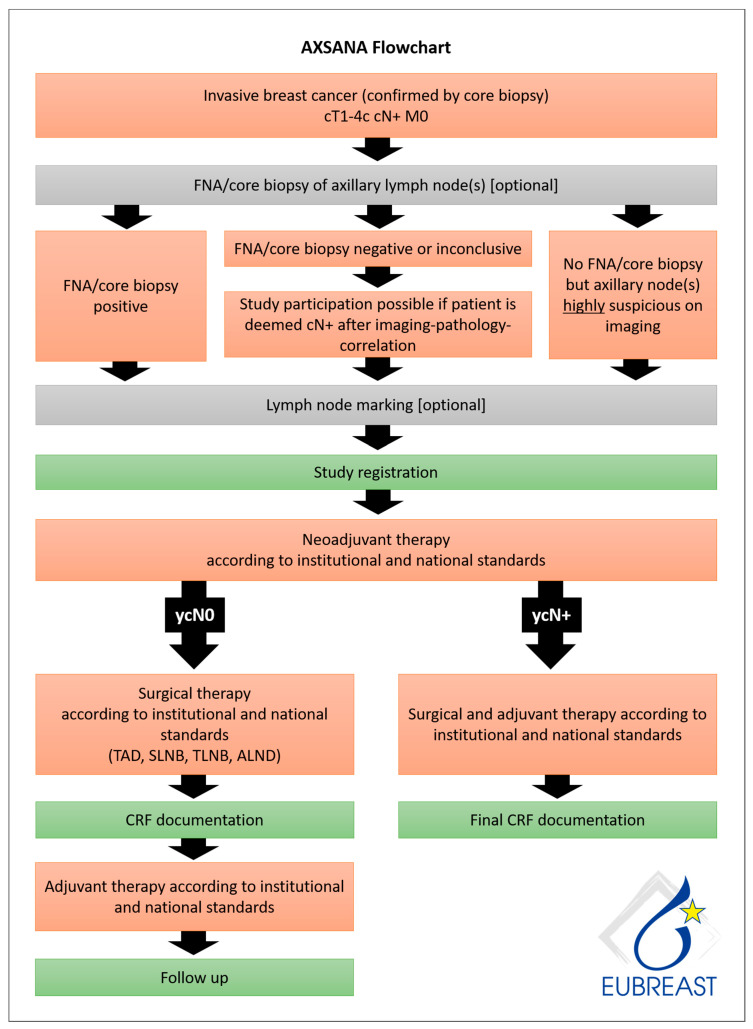
In the last two decades, surgical methods for axillary staging in breast cancer patients have become less extensive, and full axillary lymph node dissection (ALND) is confined to selected patients. In initially node-positive patients undergoing neoadjuvant chemotherapy, however, the optimal management remains unclear. Current guidelines vary widely, endorsing different strategies. We performed a literature review on axillary staging strategies and their place in international recommendations. This overview defines knowledge gaps associated with specific procedures, summarizes currently ongoing clinical trials that address these unsolved issues, and provides the rationale for further research. While some guidelines have already implemented surgical de-escalation, replacing ALND with, e.g., sentinel lymph node biopsy (SLNB) or targeted axillary dissection (TAD) in cN+ patients converting to clinical node negativity, others recommend ALND. Numerous techniques are in use for tagging lymph node metastasis, but many questions regarding the marking technique, i.e., the optimal time for marker placement and the number of marked nodes, remain unanswered. The optimal number of SLNs to be excised also remains a matter of debate. Data on oncological safety and quality of life following different staging procedures are lacking. These results provide the rationale for the multinational prospective cohort study AXSANA initiated by EUBREAST, which started enrollment in June 2020 and aims at recruiting 3000 patients in 20 countries (NCT04373655; Funded by AGO-B, Claudia von Schilling Foundation for Breast Cancer Research, AWOgyn, EndoMag, Mammotome, and MeritMedical).
在过去二十年中,乳腺癌患者腋窝分期的手术方法已变得不那么广泛,全腋窝淋巴结清扫术(ALND)仅限于特定患者。然而,对于接受新辅助化疗的初始淋巴结阳性患者,最佳治疗方案仍不明确。当前指南差异很大,支持不同的策略。我们对腋窝分期策略及其在国际建议中的地位进行了文献综述。本综述确定了与特定手术相关的知识空白,总结了目前正在进行的解决这些未解决问题的临床试验,并为进一步研究提供了理论依据。虽然一些指南已经实施了手术降级,在转为临床淋巴结阴性的cN+患者中用前哨淋巴结活检(SLNB)或靶向腋窝清扫术(TAD)取代ALND,但其他指南则推荐ALND。目前有许多技术用于标记淋巴结转移,但关于标记技术的许多问题,即标记物放置的最佳时间和标记淋巴结的数量,仍未得到解答。切除前哨淋巴结的最佳数量也仍存在争议。缺乏关于不同分期手术后肿瘤学安全性和生活质量的数据。这些结果为EUBREAST发起的多国家前瞻性队列研究AXSANA提供了理论依据,该研究于2020年6月开始招募患者,旨在在20个国家招募3000名患者(NCT04373655;由AGO-B、克劳迪娅·冯·席林乳腺癌研究基金会、AWOgyn、EndoMag、Mammotome和MeritMedical资助)。