Hao Lu, Xiang Yufeng, Liu Junhui
Department of Radiology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
Department of Orthopaedic, Linhai Second People's Hospital, Taizhou, China.
Front Surg. 2024 Jun 20;11:1406111. doi: 10.3389/fsurg.2024.1406111. eCollection 2024.
Retrospective Cohort Study.
To explore the feasibility and assess the efficacy of pedicle fixation with the Wiltse approach in the thoracic spine.
The current application of Wiltse approach is mainly practiced in the lumbar and thoracolumbar spines. Its application in the thoracic spine, however, has received little attention, especially in cases that requires only pedicel screw fixation without spinal decompression.
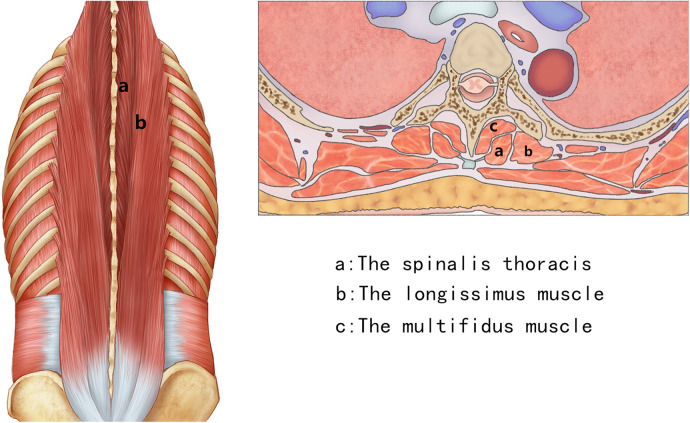
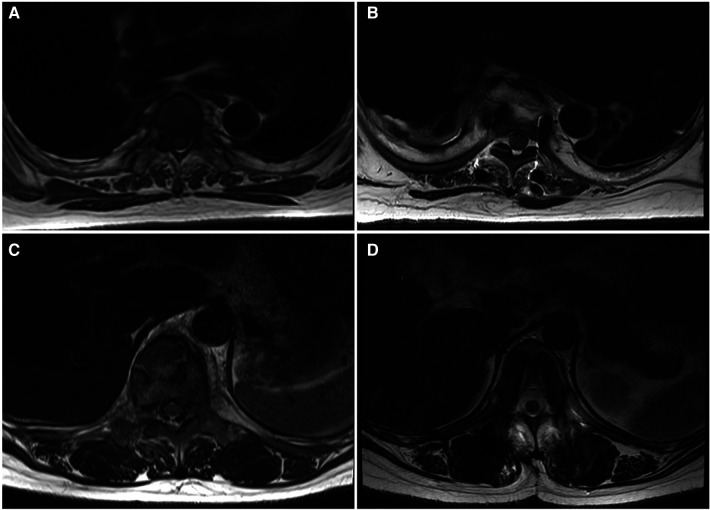
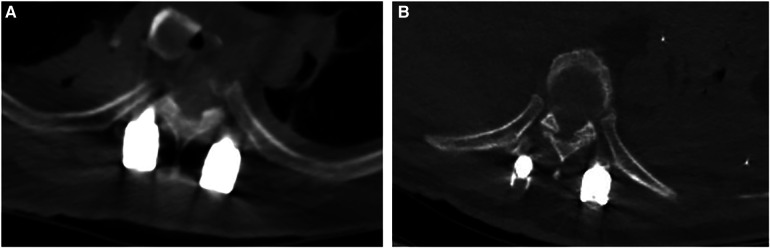
The study analyzed the clinical records of consecutive patients with thoracic diseases who underwent pedicle fixation with either Wiltse or the conventional transmuscular approach (Wiltse group: 60 cases; Transmuscular group: 48 cases). Perioperative parameters, Visual Analogue Scale (VAS) scores, accuracy of pedicle screw placement, dead space between the muscles, Magnetic Resonance Imaging (MRI) appearance, electrophysiological changes in the multifidus muscle were compared between the two groups.
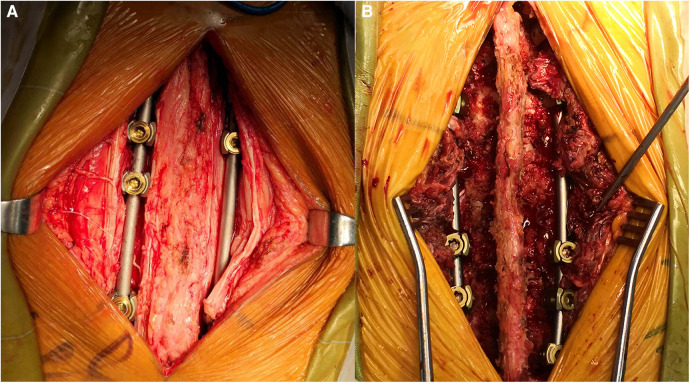
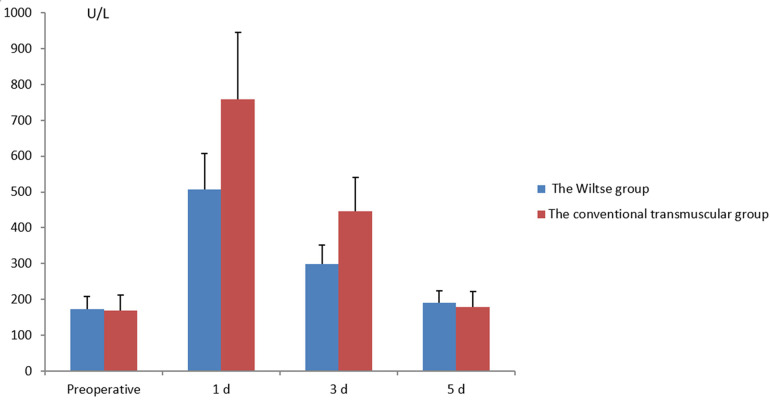
Compared with the transmuscular group, the Wiltse group was significantly better in blood loss and postoperative VAS scores. No difference was observed in incision length, operation time, and hospital stay. The dead space between the muscle cross-sectional region in the transmuscular group was 315 ± 53 mm, and no dead space was found in the Wiltse group. On MRI images, the multifidus cross-sectional area (CSA) in the Wiltse group between the preoperative period and the last follow-up reduced by only 10.1%, while transmuscular group showed 46.1% CSA reduction. Electrophysiologically, the median frequency slope of the transmuscular group grew by 47.8% with average amplitude reduced by 16.4% between the preoperative period and 12-month postoperative.
The Wiltse approach for pedicle fixation in the thoracic spine is a feasible and effective treatment, with fewer traumas and reliable clinical results. In particular, the Wiltse approach reduces postoperative dead space between the muscles and causes less atrophy in the multifidus muscle.
回顾性队列研究。
探讨采用Wiltse入路进行胸椎椎弓根固定的可行性并评估其疗效。
Wiltse入路目前主要应用于腰椎和胸腰段脊柱。然而,其在胸椎的应用很少受到关注,尤其是在仅需椎弓根螺钉固定而无需脊髓减压的病例中。
本研究分析了连续接受Wiltse入路或传统经肌入路椎弓根固定的胸椎疾病患者的临床记录(Wiltse组:60例;经肌组:48例)。比较两组的围手术期参数、视觉模拟量表(VAS)评分、椎弓根螺钉置入的准确性、肌肉间死腔、磁共振成像(MRI)表现、多裂肌的电生理变化。
与经肌组相比,Wiltse组在失血量和术后VAS评分方面明显更好。在切口长度、手术时间和住院时间方面未观察到差异。经肌组肌肉横截面积区域间的死腔为315±53 mm,而Wiltse组未发现死腔。在MRI图像上,Wiltse组术前至末次随访时多裂肌横截面积(CSA)仅减少了10.1%,而经肌组CSA减少了46.1%。电生理方面,经肌组术前至术后12个月时,中位频率斜率增长了47.8%,平均波幅降低了16.4%。
Wiltse入路用于胸椎椎弓根固定是一种可行且有效的治疗方法,创伤较小,临床结果可靠。特别是,Wiltse入路减少了术后肌肉间死腔,且多裂肌萎缩较少。