Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital, Harvard Medical School; Division of Gastroenterology and Hepatology, Department of Medicine, Massachusetts General Hospital, Harvard Medical School; and Clinical and Translational Epidemiology Unit (CTEU), Massachusetts General Hospital, Boston, Massachusetts (T.G.S.).
Division of General Internal Medicine, Department of Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts (D.E.S.).
Ann Intern Med. 2024 Aug;177(8):1028-1038. doi: 10.7326/M23-3067. Epub 2024 Jul 9.
Apixaban, rivaroxaban, and warfarin have shown benefit for preventing major ischemic events, albeit with increased bleeding risk, among patients in the general population with atrial fibrillation (AF). However, data are scarce in patients with cirrhosis and AF.
To compare the effectiveness and safety of apixaban versus rivaroxaban and versus warfarin in patients with cirrhosis and AF.
Population-based cohort study.
Two U.S. claims data sets (Medicare and Optum's de-identified Clinformatics Data Mart Database [2013 to 2022]).
1:1 propensity score (PS)-matched patients with cirrhosis and nonvalvular AF initiating use of apixaban, rivaroxaban, or warfarin.
Primary outcomes included ischemic stroke or systemic embolism and major hemorrhage (intracranial hemorrhage or major gastrointestinal bleeding). Database-specific and pooled PS-matched rate differences (RDs) per 1000 person-years (PY) and Cox proportional hazard ratios (HRs) with 95% CIs were estimated, controlling for 104 preexposure covariates.
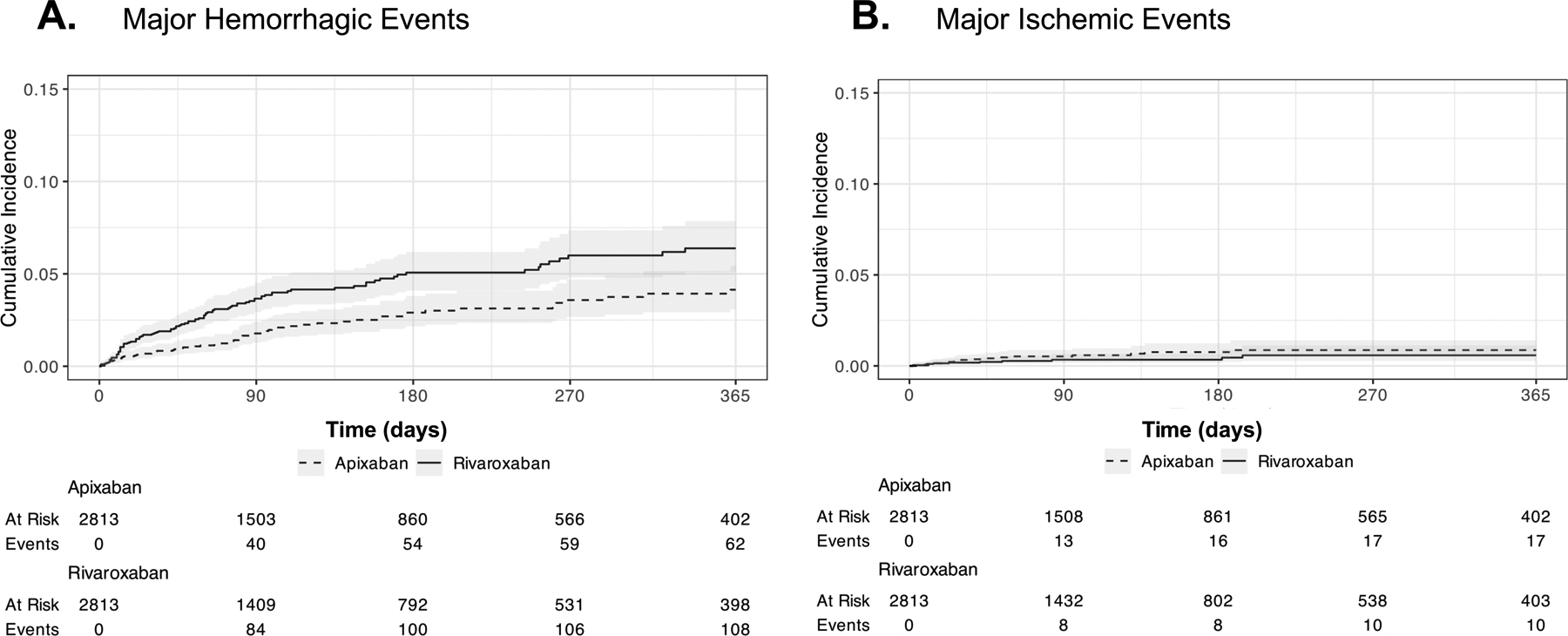
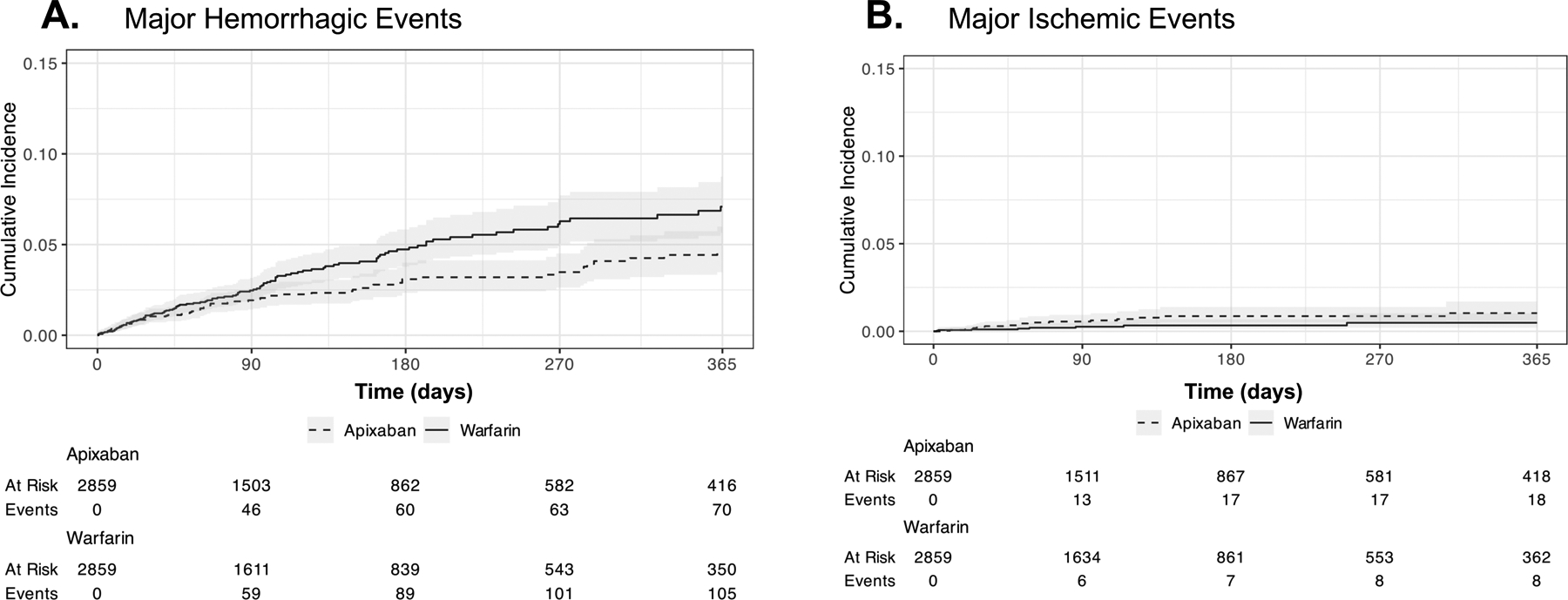
Rivaroxaban initiators had significantly higher rates of major hemorrhagic events than apixaban initiators (RD, 33.1 per 1000 PY [95% CI, 12.9 to 53.2 per 1000 PY]; HR, 1.47 [CI, 1.11 to 1.94]) but no significant differences in rates of ischemic events or death. Consistently higher rates of major hemorrhage were found with rivaroxaban across subgroup and sensitivity analyses. Warfarin initiators also had significantly higher rates of major hemorrhage than apixaban initiators (RD, 26.1 per 1000 PY [CI, 6.8 to 45.3 per 1000 PY]; HR, 1.38 [CI, 1.03 to 1.84]), particularly hemorrhagic stroke (RD, 9.7 per 1000 PY [CI, 2.2 to 17.2 per 1000 PY]; HR, 2.85 [CI, 1.24 to 6.59]).
Nonrandomized treatment selection.
Among patients with cirrhosis and nonvalvular AF, initiators of rivaroxaban versus apixaban had significantly higher rates of major hemorrhage and similar rates of ischemic events and death. Initiation of warfarin versus apixaban also contributed to significantly higher rates of major hemorrhagic events, including hemorrhagic stroke.
National Institutes of Health.
在一般人群的房颤(AF)患者中,阿哌沙班、利伐沙班和华法林在预防主要缺血性事件方面显示出益处,尽管出血风险增加。然而,在患有肝硬化和 AF 的患者中,数据仍然有限。
比较阿哌沙班与利伐沙班和华法林在患有肝硬化和 AF 的患者中的有效性和安全性。
基于人群的队列研究。
两个美国索赔数据集(医疗保险和 Optum 的去识别 Clinformatics 数据集市数据库[2013 年至 2022 年])。
1:1 倾向评分(PS)匹配的使用阿哌沙班、利伐沙班或华法林开始治疗的肝硬化和非瓣膜性 AF 患者。
主要结局包括缺血性卒中和全身性栓塞以及大出血(颅内出血或主要胃肠道出血)。估计了每 1000 人年(PY)的数据库特定和汇总 PS 匹配率差异(RD)和 Cox 比例风险比(HR)及其 95%置信区间,同时控制了 104 个暴露前协变量。
与阿哌沙班相比,利伐沙班的起始者大出血事件发生率显著更高(RD,33.1/1000 PY[95%CI,12.9 至 53.2/1000 PY];HR,1.47[CI,1.11 至 1.94]),但缺血事件或死亡的发生率没有显著差异。在亚组和敏感性分析中,利伐沙班的大出血发生率始终较高。与阿哌沙班相比,华法林的起始者也有更高的大出血发生率(RD,26.1/1000 PY[CI,6.8 至 45.3/1000 PY];HR,1.38[CI,1.03 至 1.84]),特别是出血性卒中(RD,9.7/1000 PY[CI,2.2 至 17.2/1000 PY];HR,2.85[CI,1.24 至 6.59])。
非随机治疗选择。
在患有肝硬化和非瓣膜性 AF 的患者中,与阿哌沙班相比,利伐沙班的起始者大出血发生率显著更高,而缺血事件和死亡率相似。与阿哌沙班相比,华法林的起始也会导致大出血事件发生率显著升高,包括出血性卒中。
美国国立卫生研究院。