Bart's Health National Health Service Trust, London, United Kingdom.
London's Air Ambulance, London, United Kingdom.
JAMA Surg. 2024 Sep 1;159(9):998-1007. doi: 10.1001/jamasurg.2024.2254.
Hemorrhage is the most common cause of preventable death after injury. Most deaths occur early, in the prehospital phase of care.
To establish whether prehospital zone 1 (supraceliac) partial resuscitative endovascular balloon occlusion of the aorta (Z1 P-REBOA) can be achieved in the resuscitation of adult trauma patients at risk of cardiac arrest and death due to exsanguination.
DESIGN, SETTING, AND PARTICIPANTS: This was a prospective observational cohort study (Idea, Development, Exploration, Assessment and Long-term follow-up [IDEAL] 2A design) with recruitment from June 2020 to March 2022 and follow-up until discharge from hospital, death, or 90 days evaluating a physician-led and physician-delivered, urban prehospital trauma service in the Greater London area. Trauma patients aged 16 years and older with suspected exsanguinating subdiaphragmatic hemorrhage, recent or imminent hypovolemic traumatic cardiac arrest (TCA) were included. Those with unsurvivable injuries or who were pregnant were excluded. Of 2960 individuals attended by the service during the study period, 16 were included in the study.
ZI REBOA or P-REBOA.
The main outcome was the proportion of patients in whom Z1 REBOA and Z1 P-REBOA were achieved. Clinical end points included systolic blood pressure (SBP) response to Z1 REBOA, mortality rate (1 hour, 3 hours, 24 hours, or 30 days postinjury), and survival to hospital discharge.
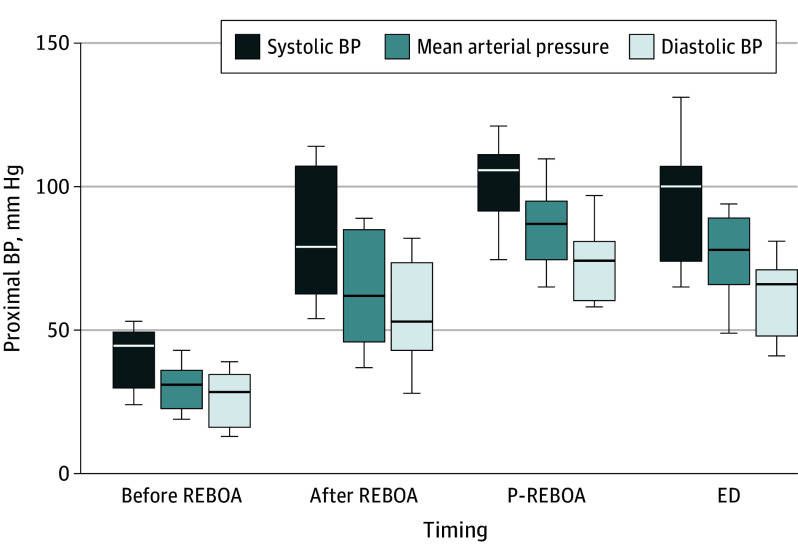
Femoral arterial access for Z1 REBOA was attempted in 16 patients (median [range] age, 30 [17-76] years; 14 [81%] male; median [IQR] Injury Severity Score, 50 [39-57]). In 2 patients with successful arterial access, REBOA was not attempted due to improvement in clinical condition. In the other 14 patients (8 [57%] of whom were in traumatic cardiac arrest [TCA]), 11 successfully underwent cannulation and had aortic balloons inflated in Z1. The 3 individuals in whom cannulation was unsuccessful were in TCA (failure rate = 3/14 [21%]). Median (IQR) pre-REBOA SBP in the 11 individuals for whom cannulation was successful (5 [46%] in TCA) was 47 (33-52) mm Hg. Z1 REBOA plus P-REBOA was associated with a significant improvement in BP (median [IQR] SBP at emergency department arrival, 101 [77-107] mm Hg; 0 of 10 patients were in TCA at arrival). The median group-level improvement in SBP from the pre-REBOA value was 52 (95% CI, 42-77) mm Hg (P < .004). P-REBOA was feasible in 8 individuals (8/11 [73%]) and occurred spontaneously in 4 of these. The 1- and 3-hour postinjury mortality rate was 9% (1/11), 24-hour mortality was 27% (3/11), and 30-day mortality was 82% (9/11). Survival to hospital discharge was 18% (2/11). Both survivors underwent early Z1 P-REBOA.
In this study, prehospital Z1 P-REBOA is feasible and may enable early survival, but with a significant incidence of late death.
ClinicalTrials.gov Identifier: NCT04145271.
出血是创伤后可预防死亡的最常见原因。大多数死亡发生在早期,即院前护理阶段。
确定在因出血导致心脏骤停和死亡风险的成人创伤患者的复苏中,是否可以实现院前区域 1(腹腔上)部分主动脉球囊阻断(Z1 P-REBOA)。
设计、地点和参与者:这是一项前瞻性观察队列研究(Idea、Development、Exploration、Assessment 和 Long-term follow-up [IDEAL] 2A 设计),于 2020 年 6 月至 2022 年 3 月期间招募,随访至患者出院、死亡或 90 天,评估伦敦大都市区的一项由医生主导和实施的城市院前创伤服务。纳入疑似腹腔下失血性、近期或即将发生失血性创伤性心脏骤停(TCA)的年龄在 16 岁及以上的创伤患者。排除无法存活的损伤或怀孕的患者。在研究期间,该服务共收治了 2960 名患者,其中 16 名患者纳入了研究。
Z1 REBOA 或 P-REBOA。
主要结果是 Z1 REBOA 和 Z1 P-REBOA 实现的患者比例。临床终点包括 Z1 REBOA 后收缩压(SBP)的反应、死亡率(受伤后 1 小时、3 小时、24 小时或 30 天)以及存活至出院。
在 16 名患者(中位[范围]年龄,30 [17-76] 岁;14 [81%] 为男性;中位数[IQR]损伤严重程度评分,50 [39-57])中尝试进行了股动脉入路的 Z1 REBOA。在 2 名动脉通路成功的患者中,由于临床状况改善,未尝试 REBOA。在其他 14 名患者(其中 8 名[57%]患有创伤性心脏骤停[TCA])中,有 11 名成功进行了套管插入并将主动脉球囊充气到 Z1。未能套管插入的 3 名患者患有 TCA(失败率=3/14 [21%])。套管插入成功的 11 名患者(5 名[TCA])的中位(IQR)预 REBOA SBP 为 47(33-52)mmHg。Z1 REBOA 加 P-REBOA 与血压的显著改善相关(到达急诊室时的中位[IQR]SBP,101[77-107]mmHg;到达时 0 名患者[TCA])。从预 REBOA 值到 SBP 的组水平平均改善为 52(95%CI,42-77)mmHg(P <.004)。在 8 名患者(8/11 [73%])中可行 P-REBOA,其中 4 名患者自发发生。受伤后 1 小时和 3 小时的死亡率为 9%(1/11),24 小时死亡率为 27%(3/11),30 天死亡率为 82%(9/11)。存活至出院的患者为 18%(2/11)。两名幸存者均早期接受了 Z1 P-REBOA。
在这项研究中,院前 Z1 P-REBOA 是可行的,可能实现早期生存,但晚期死亡率很高。
ClinicalTrials.gov 标识符:NCT04145271。