Center of Portal Hypertension, Department of Radiology, Zhongda Hospital, Medical School, Southeast University, Nurturing Center of Jiangsu Province for State Laboratory of AI Imaging & Interventional Radiology (Southeast University), Nanjing, Jiangsu, China.
Basic Medicine Research and Innovation Center of Ministry of Education, Zhongda Hospital, Southeast University, State Key Laboratory of Digital Medical Engineering, Nanjing, Jiangsu, China.
BMJ Open. 2024 Jul 11;14(7):e081623. doi: 10.1136/bmjopen-2023-081623.
Patients with clinically significant portal hypertension (CSPH) are recommended to be treated with non-selective beta-blockers (ie, carvedilol) to prevent the first hepatic decompensation event by the renewing Baveno VII consensus. CSPH is defined by hepatic venous pressure gradient (HVPG)≥10 mm Hg; however, the HVPG measurement is not widely adopted due to its invasiveness. Liver stiffness (LS)≥25 kPa can be used as a surrogate of HVPG≥10 mm Hg to rule in CSPH with 90% of the positive predicting value in majority aetiologies of patients. A compelling argument is existing for using LS≥25 kPa to diagnose CSPH and then to initiate carvedilol in patients with compensated cirrhosis, and about 5%-6% of patients under this diagnosis criteria may not be benefited from carvedilol and are at risk of lower heart rate and mean arterial pressure. Randomised controlled trial on the use of carvedilol to prevent liver decompensation in CSPH diagnosed by LS remains to elucidate. Therefore, we aimed to investigate if compensated cirrhosis patients with LS≥25 kPa may benefit from carvedilol therapy.
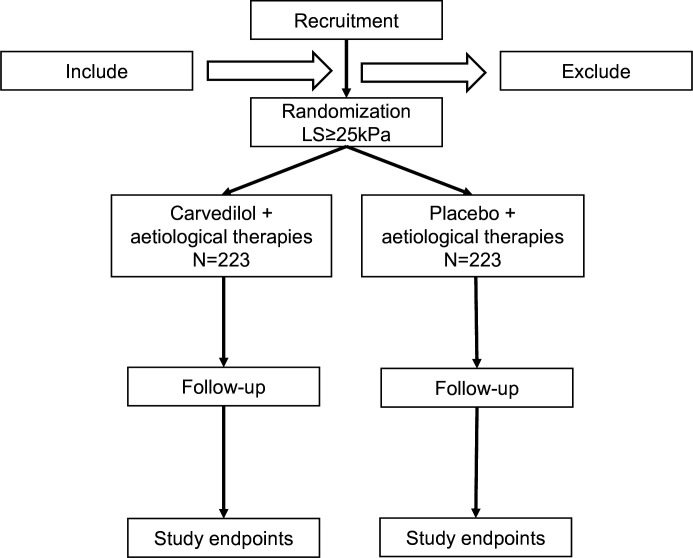
This study is a randomised, double-blind, placebo-controlled, multicentre trial. We will randomly assign 446 adult compensated cirrhosis patients with LS≥25 kPa and without any previous decompensated event and without high-risk gastro-oesophageal varices. Patients are randomly divided into two groups, with 223 subjects in group A and 223 subjects in group B. Group A is a carvedilol intervention group, while group B is a placebo group. All patients in both groups will receive aetiology therapies and are followed up at an interval of 6 months. The 3-year incidences of decompensated events of cirrhosis-related and liver-related death are the primary outcome. The secondary outcomes include development of each complication of portal hypertension individually (ascites, variceal bleeding or overt hepatic encephalopathy), development of spontaneous bacterial peritonitis and other bacterial infections, development of new varices, growth of small varices to large varices, delta changes in LS and spleen stiffness, change in hepatic dysfunction assessed by Child-Pugh and model for end-stage liver disease score, change in platelet count, development of hepatocellular carcinoma, development of portal vein thrombosis and adverse events with a 3-year follow-up. A predefined interim analysis will be performed to ensure that the calculation is reasonable.
The study protocol has been approved by the ethics committees of the Sixth People's Hospital of Shenyang (2023-05-003-01) and independent ethics committee for clinical research of Zhongda Hospital, affiliated to Southeast University (2023ZDSYLL433-P01). The results from this trial will be submitted for publication in peer-reviewed journals and will be presented at international conferences.
ChiCTR2300073864.
根据更新后的贝伐诺七共识,建议对有临床显著门静脉高压症(CSPH)的患者进行非选择性β受体阻滞剂(即卡维地洛)治疗,以预防首次肝失代偿事件。CSPH 定义为肝静脉压力梯度(HVPG)≥10mmHg;然而,由于 HVPG 测量具有侵袭性,因此并未广泛采用。肝脏硬度(LS)≥25kPa 可作为 HVPG≥10mmHg 的替代指标,用于诊断 CSPH,在大多数患者的病因中,其阳性预测值为 90%。目前有充分的证据表明,LS≥25kPa 可用于诊断 CSPH,然后在代偿性肝硬化患者中启动卡维地洛治疗,而根据这一诊断标准,约 5%-6%的患者可能无法从卡维地洛治疗中获益,并且存在心率和平均动脉压降低的风险。关于使用 LS≥25kPa 诊断 CSPH 并随后在该诊断标准下的患者中使用卡维地洛预防肝失代偿的随机对照试验仍有待阐明。因此,我们旨在研究 LS≥25kPa 的代偿性肝硬化患者是否可能从卡维地洛治疗中获益。
这是一项随机、双盲、安慰剂对照、多中心试验。我们将随机分配 446 名 LS≥25kPa 的成年代偿性肝硬化患者,这些患者无任何先前的失代偿事件,且无高危胃食管静脉曲张。患者被随机分为两组,A 组 223 例,B 组 223 例。A 组为卡维地洛干预组,B 组为安慰剂组。两组患者均接受病因治疗,并在 6 个月的间隔期进行随访。肝硬化相关和与肝脏相关的死亡的失代偿事件的 3 年发生率为主要结局。次要结局包括个别门静脉高压并发症的发展(腹水、静脉曲张出血或显性肝性脑病)、自发性细菌性腹膜炎和其他细菌感染的发展、新静脉曲张的发展、小静脉曲张进展为大静脉曲张、LS 和脾脏硬度的 delta 变化、Child-Pugh 和终末期肝病模型评分评估的肝功能障碍变化、血小板计数变化、肝细胞癌的发展、门静脉血栓形成的发展以及 3 年随访时的不良事件。将进行预设的中期分析,以确保计算合理。
该研究方案已获得沈阳第六人民医院伦理委员会(2023-05-003-01)和东南大学附属中大医院独立临床研究伦理委员会的批准。该试验的结果将提交给同行评议期刊发表,并将在国际会议上展示。
ChiCTR2300073864。