Suzuki Yuta, Kaneko Hidehiro, Okada Akira, Komuro Jin, Ko Toshiyuki, Fujiu Katsuhito, Takeda Norifumi, Morita Hiroyuki, Nishiyama Akira, Ieda Masaki, Node Koichi, Yasunaga Hideo, Nangaku Masaomi, Komuro Issei
Department of Cardiovascular Medicine, The University of Tokyo, Tokyo, Japan.
Center for Outcomes Research and Economic Evaluation for Health, National Institute of Public Health, Saitama, Japan.
Nephrol Dial Transplant. 2025 Feb 28;40(3):495-504. doi: 10.1093/ndt/gfae158.
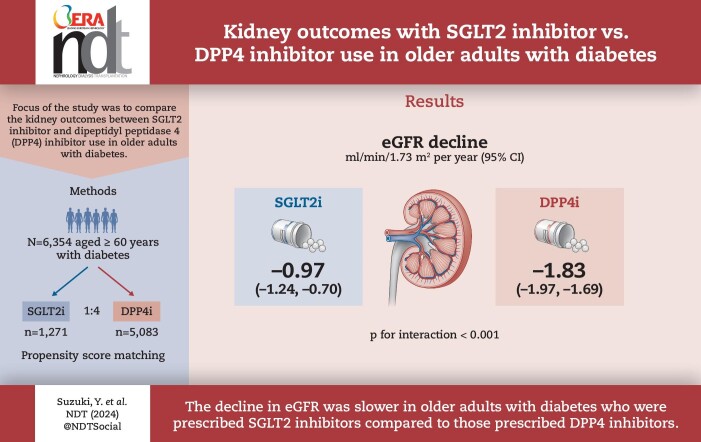
While the kidney-protective effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors have attracted much attention, there are limited real-world clinical data examining the effects of SGLT2 inhibitors on kidney function in older individuals. We aimed to compare the kidney outcomes between SGLT2 inhibitor and dipeptidyl peptidase 4 (DPP4) inhibitor use in older adults with diabetes.
Using a nationwide claims database, we studied 6354 older adults (≥60 years of age) who had diabetes and were newly initiated on SGLT2 inhibitors or DPP4 inhibitors. A 1:4 propensity score matching algorithm was used to compare changes in estimated glomerular filtration rate (eGFR) between SGLT2 inhibitor and DPP4 inhibitor users. The primary outcome was a decrease in the rate of eGFR, which was obtained using a linear mixed-effects model with an unstructured covariance.
Following propensity score matching, 6354 individuals including 1271 SGLT2 inhibitor users and 5083 DPP4 inhibitor users {median age 68 years [interquartile range (IQR) 65-70], male 60.4%, median eGFR 69.0 ml/min/1.73 m2 [IQR 59.1-79.0], median haemoglobin A1c [HbA1c] 6.9% [IQR 6.5-7.4]} were analysed. SGLT2 inhibitor users had a slower eGFR decline than did DPP4 inhibitor users [-0.97 ml/min/1.73 m2/year (95% CI -1.24 to -0.70) versus -1.83 ml/min/1.73 m2/year (95% CI -1.97 to -1.69); P for interaction <.001]. This finding remained consistent across subgroups based on age, sex, body mass index, HbA1c level, renin-angiotensin system inhibitor use and baseline eGFR. Additionally, the risk of a ≥20%, ≥30% and ≥40% decrease in eGFR from baseline was significantly lower in SGLT2 inhibitor users than in DPP4 inhibitor users.
Our analysis, utilizing a nationwide epidemiological dataset, demonstrated that the decrease in eGFR was slower in individuals ≥60 years of age with diabetes who were prescribed SGLT2 inhibitors compared with those prescribed DPP4 inhibitors, suggesting a potential advantage of SGLT2 inhibitors for kidney outcomes even in older individuals with diabetes.
虽然钠-葡萄糖协同转运蛋白2(SGLT2)抑制剂的肾脏保护作用备受关注,但关于SGLT2抑制剂对老年个体肾功能影响的真实世界临床数据有限。我们旨在比较SGLT2抑制剂和二肽基肽酶4(DPP4)抑制剂在老年糖尿病患者中的肾脏结局。
利用全国性索赔数据库,我们研究了6354名年龄≥60岁的糖尿病患者,他们新开始使用SGLT2抑制剂或DPP4抑制剂。采用1:4倾向评分匹配算法比较SGLT2抑制剂使用者和DPP4抑制剂使用者之间估算肾小球滤过率(eGFR)的变化。主要结局是eGFR下降率,通过具有非结构化协方差的线性混合效应模型获得。
倾向评分匹配后,分析了6354名个体,其中包括1271名SGLT2抑制剂使用者和5083名DPP4抑制剂使用者{中位年龄68岁[四分位间距(IQR)65 - 70],男性占60.4%,中位eGFR为69.0 ml/min/1.73m²[IQR 59.1 - 79.0],中位糖化血红蛋白[HbA1c]为6.9%[IQR 6.5 - 7.4]}。SGLT2抑制剂使用者的eGFR下降速度比DPP4抑制剂使用者慢[-0.97 ml/min/1.73m²/年(95%CI -1.24至-0.70)对-1.83 ml/min/1.73m²/年(95%CI -1.97至-1.69);交互作用P <.001]。这一发现基于年龄、性别、体重指数、HbA1c水平、肾素-血管紧张素系统抑制剂使用情况和基线eGFR的亚组分析中保持一致。此外,SGLT2抑制剂使用者从基线eGFR下降≥20%、≥30%和≥40%的风险显著低于DPP4抑制剂使用者。
我们利用全国性流行病学数据集进行的分析表明,与使用DPP4抑制剂的糖尿病患者相比,年龄≥60岁且使用SGLT2抑制剂的患者eGFR下降较慢,这表明即使在老年糖尿病患者中,SGLT2抑制剂在肾脏结局方面也具有潜在优势。