Li Tianhong, Ma Weijie, Al-Obeidi Ebaa
Division of Hematology/Oncology, Department of Internal Medicine, University of California Davis School of Medicine, University of California Davis Comprehensive Cancer Center, Sacramento, CA 95817, USA.
Medical Service, Hematology/Oncology, Veterans Affairs Northern California Health Care System, 10535 Hospital Way, Mather, CA 95655, USA.
Cancers (Basel). 2024 Jun 26;16(13):2350. doi: 10.3390/cancers16132350.
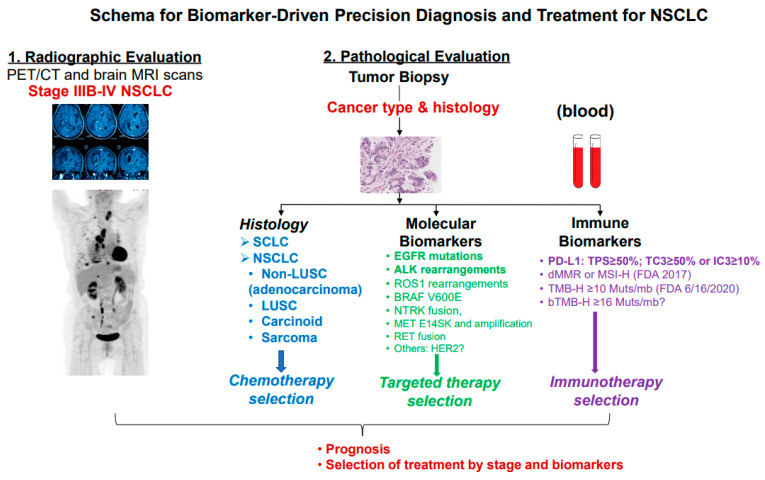
First-line systemic therapy for patients with advanced or metastatic non-small cell lung cancer (NSCLC) has rapidly evolved over the past two decades. First, molecularly targeted therapy for a growing number of molecular targets has been shown to improve progression-free survival (PFS) and overall survival (OS) with favorable toxicity profiles compared to platinum-containing chemotherapy and can be given as first-line systemic therapy in ~25% of patients with NSCLC. Actionable genetic alterations include EGFR, BRAF V600E, and MET exon 14 splicing site-sensitizing mutations, as well as ALK-, ROS1-, RET-, and NTRK-gene fusions. Secondly, inhibitors of programmed cell death protein 1 or its ligand 1 (PD-1/L1) such as pembrolizumab, atezolizumab, or cemiplimab monotherapy have become a standard of care for ~25% of patients with NSCLC whose tumors have high PD-L1 expression (total proportion score (TPS) ≥50%) and no sensitizing EGFR/ALK alterations. Lastly, for the remaining ~50% of patients who are fit and whose tumors have no or low PD-L1 expression (TPS of 0-49%) and no sensitizing EGFR/ALK aberrations, platinum-containing chemotherapy with the addition of a PD-1/L1 inhibitor alone or in combination of a cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitor improves PFS and OS compared to chemotherapy alone. The objectives of this review are to summarize the current data and perspectives on first-line systemic treatment in patients with unresectable NSCLC and propose a practical algorithm for implementing precision biomarker testing at diagnosis.
在过去二十年中,晚期或转移性非小细胞肺癌(NSCLC)患者的一线全身治疗迅速发展。首先,针对越来越多分子靶点的分子靶向治疗已被证明与含铂化疗相比,能改善无进展生存期(PFS)和总生存期(OS),且毒性特征良好,约25%的NSCLC患者可将其作为一线全身治疗。可操作的基因改变包括表皮生长因子受体(EGFR)、BRAF V600E和MET第14外显子剪接位点敏感突变,以及间变性淋巴瘤激酶(ALK)、原癌基因酪氨酸蛋白激酶ROS1(ROS1)、转染重排(RET)和神经营养酪氨酸激酶受体(NTRK)基因融合。其次,程序性细胞死亡蛋白1或其配体1(PD-1/L1)抑制剂,如帕博利珠单抗、阿替利珠单抗或西米普利单抗单药治疗,已成为约25%肿瘤具有高PD-L1表达(总比例评分(TPS)≥50%)且无敏感EGFR/ALK改变的NSCLC患者的标准治疗方案。最后,对于其余约50%身体状况良好、肿瘤无或低PD-L1表达(TPS为0-49%)且无敏感EGFR/ALK畸变的患者,与单纯化疗相比,含铂化疗联合单独使用的PD-1/L1抑制剂或与细胞毒性T淋巴细胞相关蛋白4(CTLA-4)抑制剂联合使用可改善PFS和OS。本综述的目的是总结不可切除NSCLC患者一线全身治疗的当前数据和观点,并提出一种在诊断时实施精准生物标志物检测的实用算法。